Shockwave Therapy for Athletes: Mechanisms & Latest Scientific Findings


Summary
What is shockwave therapy really, and should your athletes use it? Jim Wittstrom examines the research, explains why advice varies, and looks at which types of injuries will likely respond best to this therapeutic intervention.
The pursuit of speed, strength, and all things athletic places intense, repeated physical demands on the human body. With this highly intense demand being a prerequisite for peak athletic performance, athletes are all too familiar with incurring the various musculoskeletal injuries and disorders that can arise—the effective treatment and resolution of the underlying condition impeding performance is then of paramount importance for any serious athlete.
With the world of rehabilitative technology evolving at an ever-quickening rate and athletes looking for the quickest path back to full health, one particular intervention—known as extracorporeal shockwave therapy (ESWT), or shockwave therapy—has created quite the buzz among athletes and practitioners alike.
While this therapeutic intervention has been gaining popularity in recent years, it’s imperative for coaches, athletes, and clinicians who are considering incorporating it into their rehabilitative endeavors to have a rudimentary understanding of this modality. This includes its mechanism of action, the conditions it can treat, and, most importantly, the research behind ESWT’s ability to treat various disorders. This basic understanding is all in the name of ensuring optimal outcomes for those looking to make a full return to their athletic pursuits.
This article will walk you through these various facets pertaining to shockwave therapy, hopefully allowing you to make more informed decisions when it comes to administering or receiving shockwave therapy for your or your athlete’s needs.
How ESWT Works
While the in-depth mechanisms behind shockwave therapy are outside the scope of this article, a basic rundown is warranted for:
- How this therapy is administered.
- What shockwaves are.
- How shockwaves are believed to produce their desired effects on injured tissue.
With that said, don’t get too hung up on the details; for the average reader, knowing the scientific consensus of shockwaves’ effects on human tissue is what truly matters here (and will be discussed after this section).
Shockwave therapy has been used for treating various bone and soft tissue disorders involving the musculoskeletal system for the past 20 years.1 The process involves a handheld applicator being applied directly onto the skin over the area being treated as a series of shockwaves are administered to elicit their therapeutic effects.
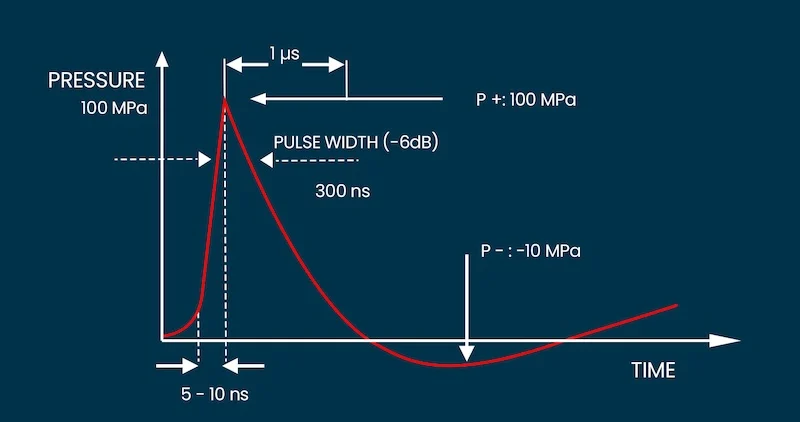
The term ‘shockwave’ is a bit of a misnomer; no electrical activity or ‘shocking’ is involved with shockwave therapy. Shockwaves are acoustic energy waves. Share on XThe term “shockwave” is a bit of a misnomer; no electrical activity or “shocking” is involved with this treatment. Shockwaves are acoustic energy waves (pressure waves) that consist of high peak-pressure amplitudes rising to their peak pressure within nanoseconds and dying out within microseconds (i.e., transient pressure oscillations).2 So, once the peak pressure of this sonic energy wave has been reached, its pressure drops to a negative value within microseconds.
As a shockwave passes through tissues within the body, its high-pressure phase can be reflected (bounce off) or absorbed by the tissue(s). As the negative phase of the shockwave interacts with these tissues, air bubbles are created in a process known as cavitation. These microbubbles then implode, leading to direct and indirect effects within the tissue(s) being targeted.3
If that sounds a bit confusing, don’t sweat it. Essentially, it’s a sonic pulse that works in the same way a fast-flying aircraft produces a sonic boom, and it leads to stimulation of human tissue at the cellular level.
More specifically, these “sonic booms” that penetrate the tissue stimulate physiological cellular activity of the targeted tissue through a process known as mechanotransduction.4,5 This fancy-sounding word simply means that a physical impulse or mechanical force is being converted into cellular activity within the targeted tissue(s).
While the specific biological changes that occur to tissue through ESWT are far outside the scope of this article, tissue regeneration through the delivery of shockwaves has been shown to occur by inducing:3,4,6,7
- Blood vessel formation (known as neovascularization).
- Growth factor release.
- Inhibition of inflammatory molecules.
- Increased tenocyte proliferation and collagen synthesis.
Additional effects have also been documented; however, the above effects are likely the primary mechanisms involved with optimizing cellular activity and health. Despite the scientific community’s general understanding of these biological changes occurring from ESWT, the exact mechanisms for how these biological and physiological responses occur are not fully understood.
Parameters of ESWT
As with any therapeutic intervention that can be implemented, shockwave therapy relies on a series of parameters that must occur to achieve the overall desired treatment effect. For the average reader, I would advise not to get hung up on these specifics; I have merely (and briefly) included them for clinicians and the curious of mind who like knowing the details of therapeutic interventions.
When treating various orthopedic disorders, shockwave parameters include:8
- Pressure distribution.
- Energy flux density.
- Total acoustic energy.
Pressure distribution refers to the area of tissue being stimulated from the shockwave being administered.
Energy flux density refers to the measure of the energy per square area that is being released by the sonic pulse at a specific point. Or, more simply put, it’s the intensity at the focal point of the shockwave. It is measured in joules of energy per area (mJ/mm2).
The extent of energy flux density can be classified as high or low; however, there is no scientific consensus on these particular definitions. It has been proposed as a guideline that low-energy ESWT involves a flux density below 0.12 mJ/mm2, while high-energy flux density is above 0.12 mJ/mm2.1
Total acoustic energy refers to the energy flux density within a single shockwave pulse multiplied by the total number of pulses administered.
Focused vs. Radial ESWT
It’s worth noting that when administering ESWT for musculoskeletal conditions, two primary types of shockwave therapy can be administered to injured tissue:
- Focused shockwave therapy.
- Radial shockwave therapy.
Focused shockwave therapy is the more “pure” or established form of shockwave therapy within the medical world. Much of the research involves studying the effects of EWST using this form of treatment.1 It involves administering shockwaves to a much more focal region of tissue, typically 2–8 millimeters in diameter.
Radial shockwaves are not concentrated directly over the targeted tissue in the same manner as focused shockwaves. Instead, the pressure waves disperse outward from the applicator tip of the device. The primary benefit is that this allows for the treatment of larger areas of tissue with less precision. However, these pressure waves do not penetrate as deep, and their characteristics are different enough that some authors contest they should not be considered true shockwaves.1,9
The existence of two different forms of shockwave therapy muddies the water when looking at the research and is a potential reason why results can vary differently across studies. Share on XWhile both forms of shockwave therapy are employed in literature and clinical settings, the existence of two different forms of ESWT muddies the water when looking at the research (this will be discussed further in the article) and is a potential reason why results can vary differently across studies.
Analyzing the Scientific Research
Enough research on ESWT has been performed that meta-analyses and systematic reviews often exist for specific orthopedic conditions. Despite this, I certainly can’t cover the findings for every condition. Rather, my aim is to skim the surface for the overall scientific findings for conditions most likely to affect the SimpliFaster audience and point those interested in further details in the right direction. For those looking to dive into the specifics of ESWT for specific orthopedic conditions (issues affecting muscles, tendons, bones, and joints), the references listed at the end of this article will serve as a solid starting point.
When analyzing the research behind ESWT’s effectiveness on various orthopedic conditions, I have tried to include findings from results and discussions within meta-analyses and systematic reviews, which offer the highest level of evidence possible within research.
Findings for Tendinopathies
Tendinopathy is one of the most commonly diagnosed conditions within athletic populations, with reports of approximately 30% of all elite athlete injuries.10 As such, findings of ESWT’s effects on tendon health should be of paramount interest to coaches and clinicians alike who are involved with athletes.
In the lower extremity, the most commonly afflicted tendons are the Achilles tendon, the plantar fascia, gluteal tendons (notably the glute medius and minimus), the patellar tendon (knee tendon), and the tibialis posterior tendon (near the inside of the ankle).11 For athletes involved in running-based sports, tendinopathy in the knee, foot, and ankle appears to be the most common.12
In the upper extremity, the rotator cuff and the flexor and extensor tendons of the elbow are most commonly affected, though I am not covering the upper extremities in this article.10
When looking at ESWT’s effects on tendinopathy, the quick takeaway is that shockwave therapy has been found to have a notable influence on reducing pain and producing health-promoting biological effects. Meta-analyses for the treatment of patellar tendinopathy, Achilles tendinopathy, and rotator cuff tendinopathy have shown statistically significant effects for various aspects of improving tendon health and function.
When looking at ESWT’s effects on tendinopathy, the quick takeaway is shockwave therapy has been found to have a notable influence on reducing pain and producing health-promoting biological effects. Share on XCritical to this topic, however, is that multiple adjunctive treatments should still be considered and implemented (when appropriate) alongside ESWT to ensure optimal tendon stimulation and subsequent healing. Which specific combined interventions lead to superior outcomes is likely best left to the clinician. The research isn’t entirely clear as to which combined intervention(s), when stacked with ESWT, will offer the best results.4
Based on our understanding of the cellular processes that arise and occur with tendon stimulation, it seems that combining ESWT with optimal tendon loading parameters will yield the best possible outcomes, though again, this depends greatly on the athlete’s condition. I have written a detailed article on SimpliFaster for the latest findings for tendon loading when treating tendinopathy, which can help provide a foundation for this approach.
Anecdotally, I will say that my patients experience far better outcomes when ESWT is paired with a loading program suitable for their needs, abilities, and overall condition. I often need to reduce training load, volume, and intensity to an appropriate level as well.
For conciseness and to appeal to the general nature of running- and sprinting-based readers on this site, I’ll only cover lower-body tendinopathy and soft tissue findings here.
Knee Tendinopathies
Overall, the findings for ESWT to produce statistically significant and favorable changes for patellar tendinopathy seem quite promising. A meta-analysis by Mani-Babu et al. reviewed seven papers examining the efficacy of ESWT on characteristics of patellar tendinopathy and found six out of seven of those papers to report significant improvement in symptoms after treatment, concluding it to be a largely successful form of conservative treatment.13
As with essentially all other systematic reviews that have analyzed the efficacy of ESWT, the review mentions that each paper utilized different shockwave parameters when providing treatment to the patellar tendon, making it difficult to determine optimal shockwave parameters when treating the condition. (This is a common theme within almost all ESWT meta-analyses dealing with soft-tissue pathologies.) The authors are quick to point out that more research is needed to determine optimal treatment parameters.
A similar meta-analysis by Liao et al. examined the effects of ESWT to reduce pain and improve functional outcomes for individuals with various soft tissue disorders of the knee (such as pes anserine tendinopathy, IT band friction syndrome, and post-traumatic tendon/ligament stiffness, among others) in addition to patellar tendinopathy.5 The results of this meta-analysis determined that ESWT showed significant moderate evidence for safety and efficacy for improving overall treatment success, reducing pain, improving functional recovery, and performance-based outcomes.5
Readers should note that in this meta-analysis, some studies utilized focused shockwave therapy while others utilized radial shockwave therapy. As such, the authors mention it is unclear whether therapeutic effects on these knee disorders differ from one shockwave form to another. (This is another common theme in many ESWT meta-analyses.)
Achilles Tendinopathy
With the Achilles tendon being one of the most adversely affected tendons in the lower body and the cornerstone of any athletic activity involving jumping and running, the effects of ESWT on this region of the body have been well studied. On the whole, meta-analyses tend to go back and forth on the efficacy of ESWT on different portions of the Achilles tendon. It would seem that some of this is due to examining various studies that largely use different shockwave parameters within each respective study.
Mani-Babu et al. concluded in their analysis that ESWT has moderate evidence for being more effective than eccentric loading for insertional Achilles tendinopathy and equal to eccentric loading for mid-portion tendinopathy. They are quick to point out that combining EWST with eccentric loading may likely produce superior outcomes.13
Similarly, a systematic review by Cathy Speed concluded that focused and radial shockwave therapy both have limited evidence to suggest they can be beneficial to insertional and mid-portion Achilles tendinopathy.1
To cloud the water even more, a meta-analysis by Fan et al. concluded through a subgroup analysis that low- and mid-energy level ESWT led to better functional outcomes and improved pain outcomes than patients who received other treatment interventions.14 They are quick to note within this paper that further investigation should take place to determine the optimal energy level of shockwave delivery.
Determining the optimal energy level of shockwave therapy is critical as it likely largely influences efficacy and outcomes when treating Achilles tendinopathy. Share on XThis last point regarding the optimal energy level of shockwave therapy is critical to understand, as it likely largely influences efficacy and outcomes when treating Achilles tendinopathy (or other tendinopathies, for that matter). A brief discussion of optimal parameters is given later in this article.
Findings for Plantar Fasciitis
An extensive volume of research on ESWT’s ability to treat plantar fasciitis has been undertaken over the past decade, with results generally finding favor in its ability to reduce pain and improve functional outcomes.
A meta-analysis by Sun et al. examining nine randomized controlled trials of ESWT on 935 patients with plantar fasciitis concluded that focused shockwave therapy could relieve pain in chronic plantar fasciitis but could not draw conclusions about radial shockwave therapy.15
In a meta-analysis with the same title, Aqil et al. concluded that ESWT produced favorable results for reducing pain in patients with chronic plantar fasciitis and recommended its use for those failing to make improvements after three months of other conservative measures.16
When determining optimal parameters, a systematic review and network meta-analysis by Chang et al. concluded that optimal delivery parameters when treating plantar fasciitis with focused shockwave therapy should involve selecting the highest tolerable energy output within a medium intensity range.17 They also concluded that radial shockwave therapy could be an appropriate alternative due to its lower price point and therapeutic effectiveness.
Other Lower Body Conditions
The research and subsequent effects of ESWT extend beyond soft tissue conditions. While not covered in this article, when pertaining to the lower body, favorable findings within meta-analyses have been found for knee osteoarthritis, acute and chronic soft tissue wounds, and medial tibial stress syndrome (shin splints), among others.18–20
Primary Advantages of ESWT
When considering treatment interventions, coaches and clinicians alike should have a preliminary understanding of the inherent risks and advantages they feel may be warranted for their athlete.
Regarding the use of ESWT for soft tissue disorders, this treatment is largely regarded as safe when used by trained professionals and can, therefore, be considered a first-line treatment option for soft tissue disorders that fail to resolve through traditional interventions. Its non-invasive nature can reduce risks that are inherent with injection-based therapies (such as infection) and surgeries.1,3,8,21
While it’s disputed whether they produce different outcomes, both focused and radial shockwave therapy are largely considered safe forms of shockwave delivery. Share on XAdditionally, ESWT is becoming more commonplace within clinical practice, adding a convenience factor for those looking to receive this treatment. Radial shockwave is typically found in clinics more often than its focused counterpart due to its more economical price point. While it’s disputed whether they produce different outcomes, both are largely considered safe forms of shockwave delivery.
Shortcoming #1: Lack of Ideal Parameter Usage
For all that we know about the effectiveness of shockwave therapy on various tissues within the body, there is a bit of the Wild West when it comes to a scientific consensus as to the ideal combination of parameters to use.4
ESWT treatment parameters often vary across studies, and there is often a surprising lack of recorded parameters (pressure distribution, energy flux density, and total acoustic energy) within studies, causing great frustration to researchers (and clinicians such as myself); a study that shows statistically significant effects on a specific condition without fully listing parameters that were selected is like providing a treasure map without a compass.
As such, it’s often up to clinicians to use anecdotal evidence to select the combination of parameters they believe to be best for the individual whom they’re treating, making for a notable shortcoming at this time when assessing the scientific strength of ESWT.
Shortcoming #2: Focused vs. Radial ESWT
As alluded to earlier, the research regarding the superiority for different orthopedic conditions when comparing focused and radial shockwave therapy is quite unclear. To further complicate matters, it has been suggested that radial shockwave is an inaccurate term and that radial pulse therapy is more accurate for various reasons.1 It has been noted by the same author that some studies involving “low energy” shockwaves are, in fact, referring to radial pulse therapy.
I make mention of this preceding paragraph to highlight a likely cause for discrepancies between randomized controlled trials examining the effectiveness of ESWT on a particular condition; not only are parameters often not reported, but the type of shockwave administered (i.e., focused versus radial) is not mentioned within certain studies.
In knowing that respective shockwaves have different characteristics (and likely therapeutic effects), treating a particular condition with radial shockwaves might not elicit favorable results, while treating the same condition with focused shockwaves might (and vice versa). This has the potential to lead to conflicting findings within the literature (and likely does).
ESWT Can Be Beneficial
While the research leaves more to be desired as to the precise mechanisms of how shockwave therapy works, which type of shockwave is most effective for a respective condition, and which set of treatment parameters will likely yield the best outcomes possible, it’s nonetheless quite clear that ESWT can offer benefits regarding tissue healing, pain reduction, and functional improvement for various orthopedic conditions.
Athletes, coaches, and clinicians looking for safe, non-invasive treatment for tendinopathies and soft tissue disorders, and potentially for bone healing, will likely experience the best results for what ESWT can offer and should consider combining this treatment with additional intervention such as physical therapy to maximize therapeutic outcomes.
References
1. Speed C. “A systematic review of shockwave therapies in soft tissue conditions: focusing on the evidence.” British Journal of Sports Medicine. 2014;48(21):1538–1542.
2. Ogden JA, Tóth-Kischkat A, and Schultheiss R. “Principles of shock wave therapy.” Clinical Orthopaedics and Related Research 1976-2007. 2001;387:8–17.
3. Wang CJ. “An overview of shock wave therapy in musculoskeletal disorders.” Chang Gung Medical Journal. 2003;26(4):220–232.
4. Ioppolo F, Rompe JD, Furia JP, and Cacchio A. “Clinical application of shock wave therapy (SWT) in musculoskeletal disorders.” European Journal of Physical and Rehabilitation Medicine. 2014;50(2):217–230.
5. Liao CD, Xie GM, Tsauo JY, Chen HC, and Liou TH. “Efficacy of extracorporeal shock wave therapy for knee tendinopathies and other soft tissue disorders: a meta-analysis of randomized controlled trials.” BMC Musculoskeletal Disorders. 208;19(1):278. doi:10.1186/s12891-018-2204-6.
6. Chao YH, Tsuang YH, Sun JS, et al. “Effects of shock waves on tenocyte proliferation and extracellular matrix metabolism.” Ultrasound in Medicine and Biology. 2008;34(5):841–852.
7. Martini L, Fini M, Giavaresi G, et al. “Primary Osteoblasts Response to Shock Wave Therapy Using Different Parameters.” Artificial Cells, Blood Substitutes, and Biotechnology. 2003;31(4):449–466. doi:10.1081/BIO-120025415.
8. Wang CJ. “Extracorporeal shockwave therapy in musculoskeletal disorders.” Journal of Orthopaedic Surgery and Research. 2012;7(1):11. doi:10.1186/1749-799X-7-11.
9. Cleveland RO, Chitnis PV, and McClure SR. “Acoustic field of a ballistic shock wave therapy device.” Ultrasound in Medicine and Biology. 2007;33(8):1327–1335.
10. Millar NL, Silbernagel KG, Thorborg K, et al. “Tendinopathy.” Nature Reviews Disease Primer. 2021;7(1):1–21.
11. Riel H, Lindstrøm CF, Rathleff MS, Jensen MB, and Olesen JL. “Prevalence and incidence rate of lower-extremity tendinopathies in a Danish general practice: a registry-based study.” BMC Musculoskeletal Disorders. 2019;20(1):239. doi:10.1186/s12891-019-2629-6.
12. Francis P, Whatman C, Sheerin K, Hume P, and Johnson MI. “The proportion of lower limb running injuries by gender, anatomical location and specific pathology: a systematic review.” Journal of Sports Science and Medicine. 2019;18(1):21.
13. Mani-Babu S, Morrissey D, Waugh C, Screen H, and Barton C. “The Effectiveness of Extracorporeal Shock Wave Therapy in Lower Limb Tendinopathy: A Systematic Review.” The American Journal of Sports Medicine. 2015;43(3):752–761. doi:10.1177/0363546514531911.
14. Fan Y, Feng Z, Cao J, and Fu W. “Efficacy of Extracorporeal Shock Wave Therapy for Achilles Tendinopathy: A Meta-analysis.” Orthopaedic Journal of Sports Medicine. 2020;8(2):1–9. doi:10.1177/2325967120903430.
15. Sun J, Gao F, Wang Y, Sun W, Jiang B, and Li Z. “Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: A meta-analysis of RCTs.” Medicine (Baltimore). 2017;96(15). Accessed January 20, 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5403108/
16. Aqil A, Siddiqui MRS, Solan M, Redfern DJ, Gulati V, and Cobb JP. “Extracorporeal Shock Wave Therapy Is Effective in Treating Chronic Plantar Fasciitis: A Meta-Analysis of RCTs.” Clinical Orthopaedics and Related Research. 2013;471(11):3645–3652. doi:10.1007/s11999-013-3132-2.
17. Chang KV, Chen SY, Chen WS, Tu YK, and Chien KL. “Comparative effectiveness of focused shock wave therapy of different intensity levels and radial shock wave therapy for treating plantar fasciitis. A systematic review of network meta-analysis.” Archives of Physical Medicine and Rehabilitation. 2012;93(7):1259–1268.
18. Hsieh CK, Chang CJ, Liu ZW, and Tai TW. “Extracorporeal shockwave therapy for the treatment of knee osteoarthritis: a meta-analysis.” International Orthopaedics. 2020;44(5):877–884. Doi:10.1007/s00264-020-04489-x.
19. Zhang L, Fu X, Chen S, Zhao Z, Schmitz C, and Weng C. “Efficacy and safety of extracorporeal shock wave therapy for acute and chronic soft tissue wounds: A systematic review and meta-analysis.” International Wound Journal. 2018;15(4):590–599. doi:10.111/iwj.12902
20. Forogh B, Karimzad Y, Babaei-Ghazani A, Janbazi L, Cham MB, and Abdolghaderi S. “Effect of extracorporeal shockwave therapy on medial tibia stress syndrome: A systematic review.” Current Orthopaedic Practice. 2022;33(4):384–392.
21. Dedes V, Stergioulas A, Kipreos G, Dede AM, Mitseas A, and Panoutsopoulos GI. “Effectiveness and safety of shockwave therapy in tendinopathies.” Materia Socio-Medica. 2018;30(2):131.

{kind=link}