Neuromuscular Integration Approach for Two Chronic Posture Issues


Summary
Dr. Samuel Lauman examines whether neuromuscular integration (NI) principles—the standard of care in lower extremity rehabilitation—can be successfully applied to the increasingly common posture issues of forward head and rounded shoulders.
The posture debate has grown among healthcare practitioners, with arguments being made for and against the validity of “poor postures” and their true impact on an individual. Regardless of which side of the fence you fall on this topic, two chronic postures have become increasingly notorious amidst a growing sedentary population—forward head posture (FHP) and rounded shoulder posture (RSP). The COVID-19 pandemic has changed work and study environments for a large number of us, and thus, there is a greater need to investigate rehabilitation specifically for these two postures.
The incidence of chronic forward head and rounded shoulder posture issues increased during the COVID-19 pandemic, leading to a greater need to investigate rehab specifically for these two postures. Share on XFor what has now become a staple of lower extremity rehabilitation, the implementation of neuromuscular integration techniques is considered the standard of care. Regardless of specific diagnosis or injury site, neuromuscular integration (NI) principles are adhered to with exercises designed to challenge an individual’s balance, proprioception, and coordination. Testing methods have even been developed to measure these attributes (which I will discuss later). Yet, we rarely see such emphasis placed on the rehabilitation of upper body dysfunctions.
Specifically, this post will be about the implementation of NI principles for the rehabilitation of these two common upper body postural dysfunctions—forward head (FHP) and rounded shoulder posture (RSP)—targeting the presentation, etiology, traditional treatment methods, and implementation of potential NI techniques.
Defining the Problem
FHP is typified by weakness in the deep cervical flexor muscles, namely the:
- Longus capitis.
- Longus colli.
- Rectus capitis anterior.
Together, these muscles function to create flexion at the atlantooccipital joint and through the cervical spine. This weakness is accompanied by overactivity of the semispinalis cervicis and capitis muscles, in particular, which leads to an anterior head protrusion, whereby an individual’s head extends forward and in front of their torso. This is colloquially referred to as text neck.
RSP presents as an upward and rounded shoulder presentation of the individual, almost causing the chest to appear concave from the elevation and anterior tilt of the scapular, and internal rotation of the scapular and humerus. This is caused by weakness in those scapular downward rotators, such as the middle and lower trapezius, as well the serratus anterior, which helps to posteriorly tilt the scapular to keep it attached to the thoracic cavity. A common compensatory component of RSP is overactivity of the:
- Upper trapezius.
- Levator scapulae.
- Pectoralis major/minor muscles.
We see these postures showing links to common presentations such as increased pain, decreased strength and range of motion, decreased upper extremity stability, reduced respiratory function, and muscle activation issues that impact the scapular kinematics. And, etiologically speaking, these postural abnormalities can be a precursor to pathologies such as temporomandibular joint dysfunction, chronic neck pain, thoracic outlet syndrome, scapular dyskinesis, and shoulder overuse injuries.
These two postural ailments present in a large number of individuals. FHP has been reported to affect 66% of healthy individuals aged 20-50 years of age, with RSP impacting anywhere from 66%-73% of individuals. The increase in sedentary lifestyle habits is often cited as a causing factor, with individuals hunched over screens and keyboards for large lengths of time. Couple this causation with the COVID-19 pandemic, which has altered the way many of us go to work or school, and the need for heightened awareness on this topic is paramount.
Identifying Solutions
Traditional rehabilitation techniques have focused on treating the presentations in isolation—strengthening the underactive muscles and stretching the overactive muscles. For FHP, this meant strengthening exercises such as the chin tuck (or “double chin”) and stretching the cervical extensors that cause that stooped head posture. The RSP treatment commonly saw strengthening of the periscapular muscles and humeral external rotators, while stretching the aforementioned overactive muscles present in RSP.
And that was it.
No postural cueing or training, no integration with functional movements, and no addressing of global muscles groups. Although positive results have been seen with this method, treating in isolation has long fallen out of favor in lower extremity rehabilitation, and I believe upper extremity postural rehabilitation should follow suit.
Treating presentations in isolation has long fallen out of favor in lower extremity rehabilitation, and I believe upper extremity postural rehab should follow suit. Share on XNeuromuscular integration approaches have clinicians adopt a more holistic approach to rehabilitation by:
- Optimizing an individual’s ability to stabilize joints and posture.
- Improving muscle activation patterns.
- Better reacting to proprioceptive changes.
This training philosophy has been shown to improve proprioception and stability and induce improvements in isokinetic strength while being used extensively in lower extremity rehabilitation.
Lower Extremity Work
Lower extremity work has routinely incorporated neuromuscular principles into rehabilitation protocols for a variety of injuries. Take anterior cruciate ligament (ACL) ruptures, for example. For exercise prescription immediately post-op, patients are often prescribed a series of open-kinetic chain exercises where they will have no weight-bearing limits. As strength, range of motion, and activation patterns improve, the patient will be progressed to weight-bearing activities such as assisted gait and balance exercises—early-stage neuromuscular integration implementation. Eventually, patients will progress to a variety of single leg tasks and plyometric exercises with a heavy focus on proprioception and limb/joint awareness—particularly, limiting knee valgus patterns.
Fast-forward to end stage rehabilitation, where many return-to-play requirements involve specific neuromuscular control tests such as the Y-balance test. The Y-balance test is an objective neuromuscular control measurement test consisting of an individual utilizing a single-leg stance to reach in three different planes of motion while satisfying certain performance requirements. The test is repeated on both involved and uninvolved limbs, and depending on the clinic or testing facility, a certain percentage of limb symmetry is required for clearance. Research has been done linking these neuromuscular asymmetries as predictors of future injury and even linking lower limb neuromuscular control to upper extremity injuries.
Upper Extremity Work
As you can see, there are clearly defined stages and instances where neuromuscular control is both trained and assessed in lower extremity rehabilitation protocols. Upper extremity neuromuscular protocols, on the other hand, are in their infancy.
An obvious limitation here is that the lower limb is used for gait and weight bearing due to our bipedal nature; as such, we cannot compare apples to apples. However, a level of stability and proprioception is required to complete activities of daily living and other sporting and performance tasks. Scapular dyskinesis testing is common to measure scapula-humeral rhythm to assess activation patterns during arm elevation tasks, and this test has specific criteria for qualification, although interpretation of these criteria is subjective in nature.
The upper quarter Y-balance test, which was developed by Gray Cook and Phil Plisky at Functional Movement Systems, is a more objective measure. It evaluates an individual’s ability to perform reaching movements while in the up position of a push-up. Similar to the lower extremity Y-balance test, participants must reach in three directions—medial, inferolateral, and superolateral—but we have to question the applicability of this test for the assessment of daily functionality and athletic performance.
Circling back to posture-based rehabilitation protocols for FHP and RSP, exercises have generally been isolated in nature, focusing on a single plane of movement and often a single muscular group to perform the movement. As such, further investigation into the implementation of neuromuscular principles for the treatment of upper extremity postural-based rehabilitation was necessary to probe the efficacy, applicability, and scope of these techniques.
Measurement Standards in the Research
Dr. David Anderson (San Francisco State University) and I performed an extensive literature search to examine this exact issue; these broad literature searches yielded 392 potential papers, which we then put through a variety of inclusion/exclusion criteria guidelines to finish with six eligible articles: four reporting on FHP and two on RSP.
Articles had to incorporate rehabilitation principles that were deemed to constitute neuromuscular integration, which was defined as utilizing rehabilitation methods that were more than just isolated strengthening and stretching techniques. This could include techniques such as proprioceptive neuromuscular facilitation (PNF) exercises, methods incorporating proprioception or stability training, and even core stability exercises to make rehabilitation more global in nature.
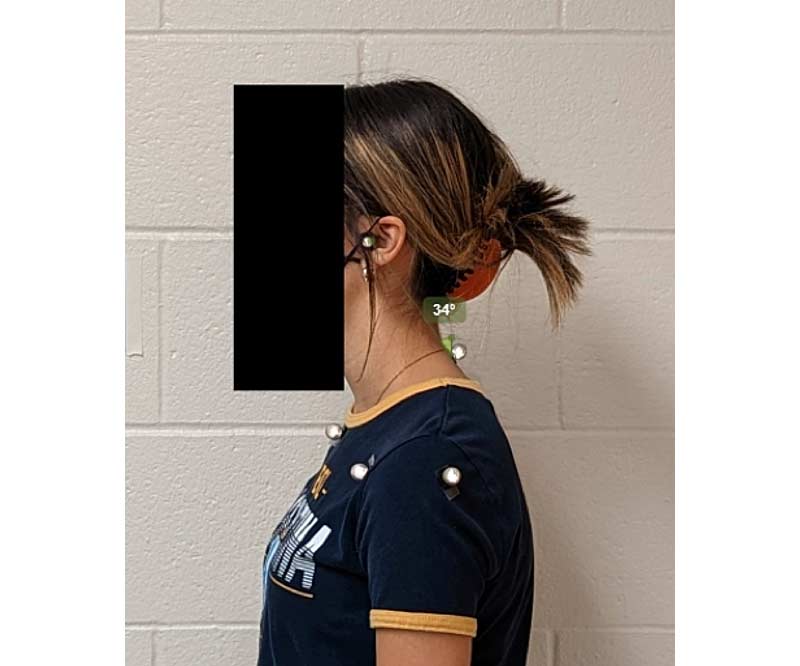
FHP is commonly measured by a technique called craniovertebral angle (CVA), which involves a subject having their photograph taken from a lateral angle, and the resultant photo is analyzed. This analysis involves two important landmarks:
- The seventh cervical vertebrae (C7).
- The tragus of the ear.
Once the photo is generated, a perpendicular line is drawn through the C7 vertebrae, and the angle from that intersection point to the tragus of the ear is measured. This process can be done manually or through a free software program such as Kinovea (used in image 1 below). CVA has been shown to be valid and reliable, and it is considered the gold standard of FHP measurement.
Unlike FHP, RSP has no gold standard measurement for practitioners to use. We have used various methods to analyze RSP, each with their own flaws. The plumb line method doesn’t account for forward torso lean originating in the lower extremity and provides a cue for participants to use and address their posture. This is referred to as the Hawthorne effect—the notion that an individual will modify their behavior when they know they are being observed. An individual can use this plumb line as a reference point for their own posture, ultimately changing their natural stance, which will impact shoulder measurement marks.
Research has also incorporated supine techniques using a table to measure the distance in which the shoulders come off the table. Obvious flaws here include the table providing a resting position for the participant whereby gravity assists them into a “better” posture, and also that this technique does not measure a posture in a way that reflects daily life.
One method that does have promise, though, is the scapular index (SI) method, which uses a tape measure to measure two distances:
- Sternal notch to coracoid process (A).
- C7 vertebrae to posterior, lateral acromion (B).
Distance (A) is divided by distance (B) and then the answer is multiplied by 100 for a raw score. This method is obviously prone to the Hawthorne effect—whereby participants know they are being measured—but from an anatomical and functional standpoint, I believe it holds the most potential to accurately measure RSP without the use of expensive or motion capture equipment.
For FHP, a combination of stabilization and strengthening exercises1–3 and a denneroll traction device were used in conjunction with neuromuscular integration techniques4. The RSP studies utilized two different methodologies: one saw investigated single bout neuromuscular stretching techniques5, and the other implemented FHP techniques to measure their effects on RSP6.
There is one key limitation to this study’s findings: we have an established method of posture measurement for FHP, but no gold standard for RSP. There is a large need for universality when it comes to accurately and reliably measuring this posture.
The Results
Neuromuscular integration approaches were shown to be beneficial for the treatment of FHP in three out of four studies, regardless of the delivery style for the neuromuscular integration principles. One study saw improvements in CVA and respiratory function through the use of McKenzie techniques, another saw improvements in CVA with a combination of neuromuscular techniques and traction, and the third successful study used DNS techniques to yield CVA results (with the unsuccessful study being the shortest intervention period of only four weeks).
The two studies looking at RSP, however, varied in their methods for measuring RSP. One study was an acute intervention with post-testing occurring immediately after the single bout of exercise, and the other study implemented FHP-specific exercises to see the impact they had on RSP. The immediate intervention group split 40 participants into four groups with varying stretching and release techniques. Of these, the group that utilized contract-relax PNF techniques saw significant variance in pectoralis minor index scores (a measure of RSP).
Takeaways
A neuromuscular integration approach to the treatment of postural disorders provides mixed results and needs to be investigated further. Evidence suggests that such techniques are effective for FHP, but such efficacy is left to be desired for RSP. The lack of results for RSP interventions could at least partially be explained by the limitation listed earlier: lack of uniformity in testing procedures.
Promising results for FHP patients provides the rationale to further investigate the role neuromuscular integration techniques can plan on the alleviation of upper body disorders. Share on XExamining the correlations postural dysfunction can have on physiological components, such as breathing and cardiovascular measures, further highlights the importance of correct diagnosis of these postures separate to the functional ramifications. Promising results for FHP patients provide the rationale to further investigate the role neuromuscular integration techniques can play on the alleviation of upper body disorders. As more valid and reliable RSP measurement techniques become available, we envision similar trends.
References
1. Bae, W.-s., Lee, K.-C., and Lee, D.-Y. “The Effects of Dynamic Neuromuscular stabilization Exercise on Forward Head Posture and Spine Posture.” Medico Legal Update. 2019;19(2):670–675.
2. Kim, S., Jung, J., and Kim, N. “The effects of McKenzie exercise on forward head posture and respiratory function.” The Journal of Korean Physical Therapy. 2019;31(6):351–357.
3. Szczygiel, E., Blaut, J., Zielonka-Pycka, K., et al. “The Impact of Deep Muscle Training on the Quality of Posture and Breathing.” Journal of Motor Behavior. 2018;50(2):219–227.
4. Moustafa, I.M., Diab, A.A., Hegazy, F., and Harrison, D.E. “Does improvement towards a normal cervical sagittal configuration aid in the management of cervical myofascial pain syndrome: a 1-year randomized controlled trial.” BMC Musculoskeletal Disorders. 2018;19(1):396.
5. Birinci, T., Mustafaoglu, R., Kaya Mutlu, E., and Razak Ozdincler, A. “Stretching exercises combined with ischemic compression in pectoralis minor muscle with latent trigger points: A single-blind, randomized, controlled pilot trial.” Complementary Therapies in Clinical Practices. 2020;38:101080.
6. Do Youn Lee, C.W.N., Sung, Y.B., Kim, K., and Lee, H.Y. “Changed in rounded shoulder posture and forward head posture according to exercise methods.” Journal of Physical Therapy Science. 2017;29(10):1824–1827.

{kind=link}