How S&C Coaches Can Assess Thoracic Spine & Upper Extremity Mobility

In this Article
- Using a Smartphone to Perform ROM Assessments
- Palpating Bony Landmarks
- Thoracic Spine Extension Test
- Lumbar Locked Rotation Test
- Supine Active Shoulder Flexion Test
- Pectoralis Major Length Test
- Supine Active Shoulder Rotation Test
- Weight-Bearing Wrist Extension Test
- Reliability of Tests
- What to Do Next?
- References

Summary
Part 2 of a two-part series on mobility assessment addresses the thoracic spine and upper extremities. As with part 1, Coach Louis Howe explains how to calibrate and use a smartphone for measurements. He also demonstrates how to perform six specific tests and collect objective data on them.
As mobility is a key physical quality that underpins most athletic movements, strength and conditioning coaches must possess the skill set and tools to assess it. Conventionally, range of motion (ROM) tests have been performed using specialized equipment such as inclinometers and goniometers. To make the execution of these tests even more challenging for coaches, many ROM assessments require exceptional palpatory skills. This has resulted in many resources suggesting an approach to mobility testing that employs a pass-fail criterion (e.g., if an athlete can’t touch their toes during a toe-touch test, they fail the test).
Yet, this method of assessing mobility has major limitations. If an athlete fails the standard set, we have obviously identified a deficiency is present—this is where a pass-fail criterion for a ROM assessment is applicable. However, if we want to monitor the effectiveness of our training intervention and identify what strategies actually develop mobility, we need assessment techniques that provide objective data that is accurate and reliable.
To monitor the effectiveness of your training intervention and identify what strategies develop mobility, you need assessment techniques that provide objective, accurate, reliable data. Share on XThe goal of this two-part article series is to demonstrate that neither the availability of equipment nor the palpatory skills a practitioner possesses should prevent coaches from collecting objective data. Part 1 of this series demonstrated how to perform mobility assessments for the lower extremity. In part 2 (this article), I will focus on mobility tests for the thoracic spine and upper extremity, showing techniques using only a smartphone or tape measure. In particular, I’ll explain and demonstrate how to perform and collect objective data for the following tests:
- Thoracic spine extension test
- Lumbar locked rotation test
- Supine active shoulder flexion test
- Pectoralis major length test
- Supine active shoulder rotation test (external and internal)
- Weight-bearing wrist extension test
Following the demonstration of each test, this article will present reliability data for all of the assessments discussed in both parts of this series to support coaches’ interpretations.
Using a Smartphone to Perform ROM Assessments
For most of the tests presented, a smartphone will be used to measure segment angles. Before we discuss techniques for measuring thoracic and upper extremity mobility, it is important we establish how to standardize our testing procedures when using a smartphone for ROM assessments. This is repetition from the first article, so feel free to skip this section if you have read the lower limb edition of this series. If you didn’t, here are considerations for collecting reliable data:
- If present, remove the phone case. It is possible the case may alter the contour of the phone.
- Before testing, calibrate the phone against either a vertical (e.g., wall) or horizontal (e.g., table) reference point. This should be done against a surface that is level, so be sure to check before calibration by placing a spirit level on the surface. Not all free applications allow you to zero the smartphone, which should be a consideration when selecting an application to perform ROM assessments. Whether you need to calibrate the smartphone against a vertical or horizontal surface depends on the test used and is described in the procedures for each assessment.
- I also recommend coaches be cautious about using different phone models interchangeably. At present, there isn’t much evidence for this to be a concern, but until quality research is presented, I suggest you perform all tests using the same model.
- Again, there is little evidence for this, but I would recommend caution using different applications interchangeably.
Palpating Bony Landmarks
An important consideration for collecting reliable data is being able to locate anatomical landmarks for measuring segment alignment. For two of the tests shown in this article, coaches will need to be able to palpate the olecranon process of the ulnar (figure 1).

Palpating the spinous processes can be a particular issue for assessing spine ROM. Although learning how to palpate specific spinal segments isn’t too difficult, it’s not the easiest skill to teach on this platform. For other assessments, measuring joint alignment can be tricky due to the nature of the assessments. To get around these issues, coaches can record distances between various structures using a tape measure to represent joint ROM. An example of this approach is the weight-bearing lunge test for the ankle joint, where the toe-to-wall distance is measured to represent dorsiflexion capacity.
Although this is a very reliable measure1, one problem with this strategy is it can be challenging to establish a deficit. For example, if we know the ankle dorsiflexes to approximately 40 degrees during the back squat2, then I would want to see an athlete achieve >40 degrees during the weight-bearing lunge test. But if I’m measuring ankle ROM using the toe-to-wall distance, how do I know if an athlete with 9 centimeters has enough mobility to squat to full depth without compensations?
This is where measuring distances can be a problem. To resolve this, we can combine our measure of distance with a pass-fail criterion. This allows us to collect objective data that is reliable, while being able to identify the presence of a mobility deficit.
Thoracic Spine Extension Test
During shoulder elevation, thoracic spine extension occurs to facilitate scapulothoracic upward rotation and posterior tilt.3Although thoracic spine contribution to overhead exercises is small relative to the shoulder complex4, suboptimal thoracic spine alignment during overhead movements can hamper ROM and strength capacities for the shoulder musculature.5
To measure thoracic spine extension mobility using equipment such as an inclinometer or a smartphone, practitioners would need to palpate the cervicothoracic and thoracolumbar junctions.6This is a time-consuming process and requires a specific skill set that many coaches do not possess. To circumvent this issue, measuring the tragus-to-wall distance during the thoracic spine extension test can provide us with an objective score representing extension capacity.7
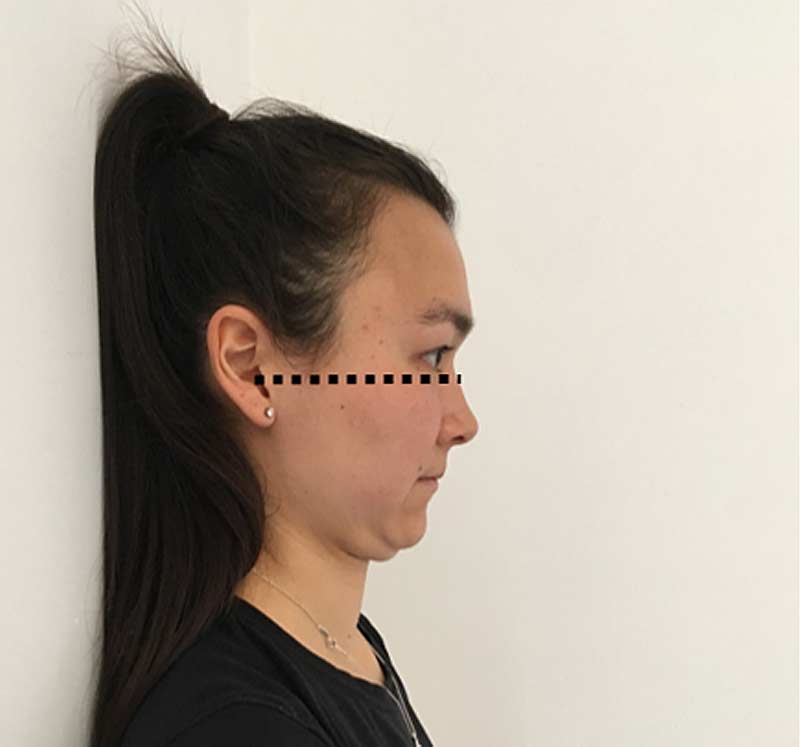
For this test, a score of <10 centimeters is generally used to represent sufficient thoracic spine extension ROM.7However, factors such as maturation, periods of weight loss/gain, and anthropometric dimensions may impact the applicability of this threshold.8To overcome this limitation, I recommend using a pass-fail criterion to support the interpretation of this test. To pass the test, the athlete should be able to bring the bottom of the inferior margin of the orbital (eye socket) to horizontally align with the auditory meatus (ear hole) while maintaining contact between the occiput and the wall (figure 2).
Starting position: The athlete leans back against the wall with their feet hip-width apart and a foot length from the wall. The knees should be slightly flexed to allow the pelvis to posteriorly rotate and the lumbar spine to flatten against the wall. The head should touch the wall and the mouth should be closed.
Movement: The athlete is cued to pull their chin toward their chest as far as possible while maintaining a closed mouth and keeping contact between the head and the wall.
Measurement: At the point where the athlete has maximally flexed the upper cervical spine to bring the chin to the chest, use a tape measure or ruler to record the distance between the tragus and the wall to the nearest 0.5 centimeters. To avoid the need to Google “tragus,” it’s the semi-circular flap that covers the auditory meatus.
Video 1. Head position is important in sport, and measuring the positioning matters. With a few cues, a test can be done in seconds. Coaches can track the changes to head position and see if those changes are factoring in sport through careful analysis.
Lumbar Locked Rotation Test
The lumbar locked rotation test isolates the thoracic spine and its capacity to rotate.9Thoracic spine rotation is important for overhead and rotational sports.10Prior to measuring thoracic spine rotation, I suggest you measure extension ROM. This is because a flexed posture tenses the posterior ligamentous structures, potentially limiting thoracic spine rotation.11
An athlete with poor thoracic spine extension & rotation should focus on increasing sagittal plane capacity first, before switching the emphasis to improving thoracic spine rotation. Share on XUnderstanding this can help from a programming perspective. An athlete who has poor thoracic spine extension and rotation should focus on increasing sagittal plane capacity first, before switching the emphasis to improving thoracic spine rotation. For this test, approximately 40 degrees relative to vertical is reported in healthy populations,12 although rotational athletes may require more thoracic spine mobility.
Starting position: The athlete kneels with the legs together and the ankles plantar flexed. The athlete rests on their forearms with the shoulder and elbows flexed to 90 degrees. With the head in a neutral position, the athlete is cued to “lift their chest.” The athlete is then instructed to bring one arm off the ground and lift the hand so it touches the sternum.
Movement: The athlete is asked to maximally rotate to the side with the arm off the ground.
Measurement: Prior to testing, the smartphone should be calibrated relative to a vertical reference point. At the point of maximal rotation, the phone is placed at the cervicothoracic junction (see figure 3). Although palpating this anatomical location requires some amount of skill, it is generally located at the level of the neckline (think crew-cut T-shirt). In my experience, using this reference point allows you to collect a reliable measure of thoracic spine rotation without the need to palpate the specific spinal level.

Video 2. Taking a position on the knees reduces the load to the spine and improves the evaluation. Rotation of the spine is essential to many sports and normal human movement.
Supine Active Shoulder Flexion Test
Shoulder flexion ROM is fundamental to most overhead exercises.4Athletes who lack shoulder flexion ROM tend to compensate by hyperextending at the lumbar spine during vertical pushing and pulling exercises. Approximately 180 degrees of shoulder flexion should be available to the healthy athlete.13As the smartphone for this test is calibrated to a vertical reference, a value of 90 degrees represents 180 degrees of shoulder flexion ROM.
Shoulder flexion ROM is fundamental to most overhead exercises, and healthy athletes should have approximately 180 degrees of shoulder flexion, says @LouisHowe_SandC. Share on XStarting position: The athlete lies supine with the knees flexed to 90 degrees and the soles of the feet flat against the ground. The athlete is cued to posteriorly rotate their pelvis to flatten the lumbar spine and prevent excessive spinal contribution. The shoulder is flexed to 90 degrees with the elbows extended and the hands facing each other.
Movement: The athlete is cued to reach the arms above the head toward the ground, keeping the elbows extended with the shoulder remaining in the sagittal plane. Coaches should monitor the athlete’s pelvic position to ensure spinal compensations do not inflate scores.
Measurement: Prior to testing, the smartphone should be calibrated relative to a vertical reference point. At maximal shoulder flexion, the smartphone is placed beneath the medial epicondyle, along the triceps muscle.
Video 3. Positioning an athlete on their back is useful for a range of motion testing. The upper back and shoulders can respond favorably to flexibility and targeted strength training.
Pectoralis Major Length Test
For this test, we measure horizontal abduction from an abducted position. Due to the architecture of the muscle, the sternocostal portion of the pectoralis major muscle is one of the primary structures that resists this motion. The length of the pectoralis major can influence the ability to optimally position the barbell during the overhead squat or the catch phase of the snatch.
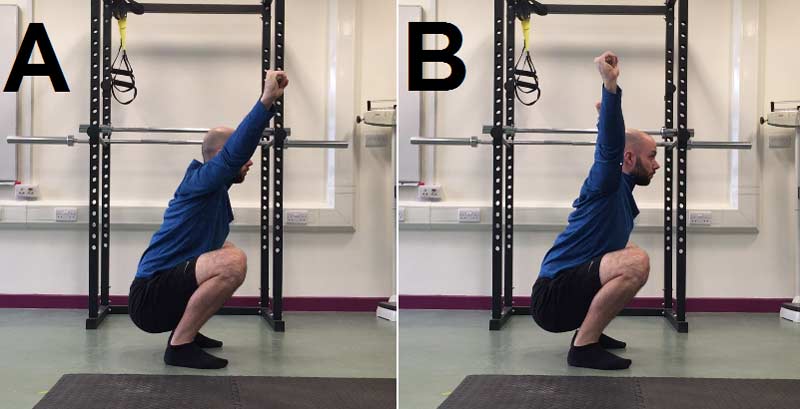
If an athlete holds the bar above their head with a snatch grip, the shoulder complex will be abducted to approximately 135 degrees. As the athlete descends, the trunk will incline forward, requiring a small amount of horizontal abduction to occur to maintain the bar path within the base of support. If this motion is not available, the athlete will struggle to keep the bar above the head. This is demonstrated in figure 4.
I haven’t seen any research establishing the clinometric properties of the test. However, I have found this test to be highly reliable. An athlete passes the pectoralis major length test when they are able to comfortably rest the arm on the ground.
Starting position: The athlete lies supine with the knees flexed to 90 degrees and the soles of the feet flat against the ground. The athlete is cued to posteriorly rotate the pelvis to flatten the lumbar spine and prevent excessive spinal contribution. The athlete is cued to make a fist with both hands and bring the knuckles together directly above the head.
Movement: The athlete is cued to draw the elbows to the floor.
Measurement: At maximal horizontal abduction, the coach assesses whether the upper arm can comfortably contact the ground. In instances where there is space between the arm and the ground, the athlete has failed the test and the coach measures the distance between the olecranon process and the ground to the nearest 0.5 centimeters.
Video 4. The pectoralis length test is a conventional evaluation with objective measurement. While not a screen for injury risk, coaches and therapists should treat each athlete individually.
Supine Active Shoulder Rotation Test
The supine active shoulder rotation test provides an insight into the mobility of the external and internal rotators of the glenohumeral joint. Normative data for these tests in resistance-trained athletes have been reported as approximately 105 degrees external rotation and 70 degrees internal rotation when measuring forearm alignment relative to vertical.13However, these values may differ in throwing athletes, with structural adaptations influencing shoulder rotation capacity in throwers.14Therefore, it may be that total rotation (external and internal rotation combined) is of greater relevance when looking to identify mobility deficits.15
Starting position: The athlete lies supine on a treatment table, with the knees flexed to 90 degrees and the feet flat on the table. The pelvis is posteriorly rotated to prevent compensations at the spine. The shoulder is abducted to 90 degrees, with the elbow flexed 90 degrees.
Movement: For external rotation, the athlete is cued to bring the back of the hand toward the ground. Conversely, the athlete is instructed to bring the palm of the hand toward the ground for internal rotation.
Measurement: Prior to testing, the smartphone should be calibrated relative to a vertical reference point. For external rotation, the smartphone is placed just below the wrist crease of the anterior side of the forearm. Internal rotation is measured by placing the smartphone on the posterior surface of the forearm, just below the wrist crease.
Video 5. Internal and external rotators of the shoulders are important for all athletes, not just overhead competitors. Soccer and other sports tend to view overhead lifting as not sport specific (except with goalkeepers), but the entire body must be optimized for peak performance.
Weight-Bearing Wrist Extension Test
I’ve included this test here, as wrist extension can be a problem during front squats or the catch position of the clean.16Normal wrist extension is considered to be approximately 95 degrees.16As forearm alignment for this test is measured relative to vertical, a value of >5 degrees for this test represents sufficient wrist extension ROM.
Wrist extension can be a problem during front squats of the catch position of the clean. Normal wrist extension should be approximately 95 degrees, says @LouisHowe_SandC. Share on XStarting position: The athlete stands in a staggered stance next to a box or table with a solid surface that is approximately mid-thigh height. The athlete places the hand so the palm is flat on the box with the fingers facing forward of the athlete.
Movement: Keeping the palm flat on the box/table with the elbow extended, the athlete is instructed to maximally move the shoulder over the hand, causing wrist extension.
Measurement: Prior to testing, the smartphone should be calibrated relative to a vertical reference point. The phone is placed beneath the olecranon process, along the ulnar on the posterior surface of the forearm.
Video 6. The wrist joint is an important part of gripping and overhead actions. Testing the wrist is a useful screen for all athletes, not just those who grip sport implements.
Reliability of Tests
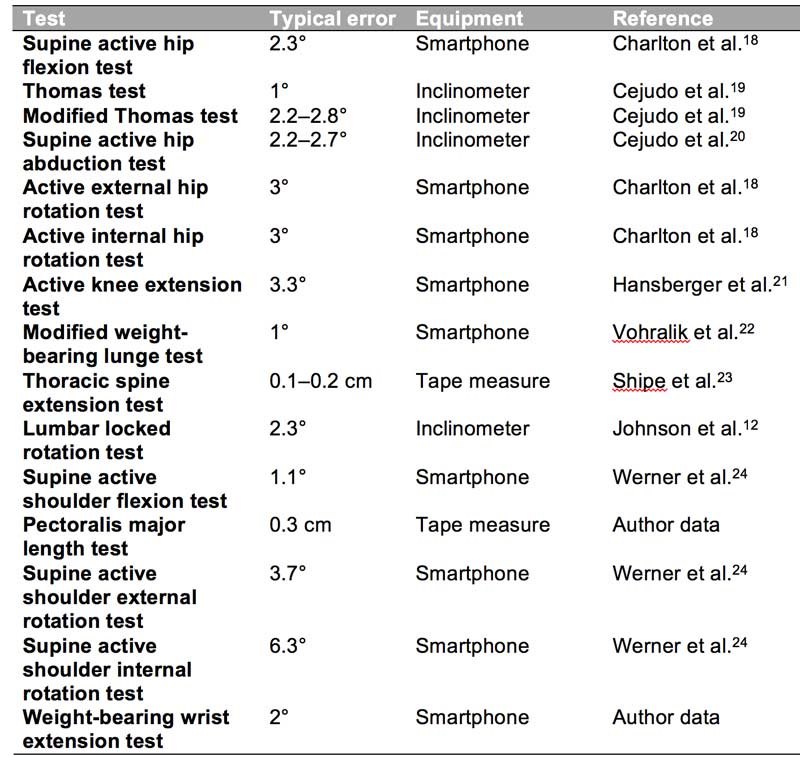
To support the interpretation of the findings from any assessment, it is very important that coaches appreciate the error associated with each test. Fortunately, many of the tests introduced in this two-part series have been extensively studied. Table 1 below provides the typical error values for each test along with the corresponding reference.
Not all of the data presented was collected using a smartphone to determine the clinometric properties of the assessment, so I’ve included a column indicating the equipment used for each study. As some of the data presented below has been collected using other equipment (i.e., inclinometer), coaches should interpret these values with caution. Furthermore, I’ve included my own between-session reliability data for two tests where no information (to my knowledge, at least) is available from the literature.
Due to some of these limitations, I recommend coaches use the table purely as a guide. In fact, because this data was collected by researchers with a different skill set than your own, using a population that likely differs from the athletes you work with, I suggest you establish your own reliability data for each test using the statistical procedures outlined by Spence and Cushion.17
What to Do Next?
As you now know how to perform the tests and have some idea as to the reliability of each test, you possess the skill set required to identify deficits. Additionally, you also have the capability to determine what mobility exercises and dosages work when it comes to improving ROM. This will likely be a pretty interesting experience for many coaches, and will no doubt help you refine your toolbox for truly developing an athlete’s mobility.
References
1. Langarika-Rocafort, A., Emparanza, J. I., Aramendi, J. F., Castellano, J., and Calleja-González, J. (2017). “Intra-rater reliability and agreement of various methods of measurement to assess dorsiflexion in the Weight Bearing Dorsiflexion Lunge Test (WBLT) among female athletes.” Physical Therapy in Sport, 23, 37–44.
2. Swinton, P. A., Lloyd, R., Keogh, J. W., Agouris, I., and Stewart, A. D. (2012). “A biomechanical comparison of the traditional squat, powerlifting squat, and box squat.” Journal of Strength and Conditioning Research, 26(7), 1805–1816.
3. Crosbie, J., Kilbreath, S. L., Hollmann, L., and York, S. (2008). “Scapulohumeral rhythm and associated spinal motion.” Clinical Biomechanics, 23(2), 184–192.
4. McKean, M. R. and Burkett, B. J. (2015). “Overhead shoulder press – In-front of the head or behind the head?” Journal of Sport and Health Science, 4(3), 250–257.
5. Kebaetse, M., McClure, P., and Pratt, N. A. (1999). “Thoracic position effect on shoulder range of motion, strength, and three-dimensional scapular kinematics.” Archives of Physical Medicine and Rehabilitation, 80(8), 945–950.
6. Lewis, J. S., Green, A., and Wright, C. (2005). “Subacromial impingement syndrome: the role of posture and muscle imbalance.” Journal of Shoulder and ElbowSurgery, 14(4), 385–392.
7. Bohannon, R. W., Tudini, F., and Constantine, D. (2019). “Tragus-to-wall: A systematic review of procedures, measurements obtained, and clinimetric properties.” Journal of Back and Musculoskeletal Rehabilitation, (Preprint), 1–11.
8. Ozaras, N., Gulec, M. G., Celik, H. K. A., Demir, S. E., and Guler, M. (2014). “Effect of body shape on tragus-to-wall distance in the normal population.” Clinical Rheumatology, 33(8), 1169–1171.
9. Bucke, J., Spencer, S., Fawcett, L., Sonvico, L., Rushton, A., and Heneghan, N. R. (2017). “Validity of the digital inclinometer and iphone when measuring thoracic spine rotation.” Journal of Athletic Training, 52(9), 820–825.
10. Young, J. L., Herring, S. A., Press, J. M., and Casazza, B. A. (1996). “The influence of the spine on the shoulder in the throwing athlete.” Journal of Back and Musculoskeletal Rehabilitation, 7(1), 5–17.
11. Edmondston, S. J., Aggerholm, M., Elfving, S., Flores, N., Ng, C., Smith, R., and Netto, K. (2007). “Influence of posture on the range of axial rotation and coupled lateral flexion of the thoracic spine.” Journal of Manipulative and Physiological Therapeutics, 30(3), 193–199.
12. Johnson, K. D., Kim, K. M., Yu, B. K., Saliba, S. A., and Grindstaff, T. L. (2012). “Reliability of thoracic spine rotation range-of-motion measurements in healthy adults.” Journal of Athletic Training, 47(1), 52–60.
13. Barlow, J. C., Benjamin, B. W., Birt, P. J., and Hughes, C. J. (2002). “Shoulder strength and range-of-motion characteristics in bodybuilders.” Journal of Strength and Conditioning Research, 16(3), 367–372.
14. Reagan, K. M., Meister, K., Horodyski, M. B., Werner, D. W., Carruthers, C., and Wilk, K. (2002). “Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players.” The American Journal of Sports Medicine, 30(3), 354–360.
15. Wilk, K. E., Macrina, L. C., Fleisig, G. S., Porterfield, R., Simpson, C. D., Harker, P., Paparesta, N., and Andrews, J. R. (2011). “Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers.” The American Journal of Sports Medicine, 39(2), 329–335.
16. Bousquet, B. A. and Olson, T. (2018). “Starting at the Ground Up: Range of Motion Requirements and Assessment Procedures for Weightlifting Movements.” Strength and Conditioning Journal, 40(6), 56–67.
17. Spence, A. and Cushion, E. (2015). “Determining reliability: a data collection guide for S&C practitioners.” Professional Strength and Conditioning Journal, 36, 27–33.
18. Charlton, P. C., Mentiplay, B. F., Pua, Y. H., and Clark, R. A. (2015). “Reliability and concurrent validity of a Smartphone, bubble inclinometer and motion analysis system for measurement of hip joint range of motion.” Journal of Science and Medicine in Sport, 18(3), 262–267.
19. Cejudo, A., de Baranda, P. S., Ayala, F., and Santonja, F. (2015). “Test-retest reliability of seven common clinical tests for assessing lower extremity muscle flexibility in futsal and handball players.” Physical Therapy in Sport, 16(2), 107–113.
20. Cejudo, A., Ayala, F., De Baranda, P. S., and Santonja, F. (2015). “Reliability of two methods of clinical examination of the flexibility of the hip adductor muscles.” International Journal of Sports Physical Therapy, 10(7), 976.
21. Hansberger, B. L., Loutsch, R., Hancock, C., Bonser, R., Zeigel, A., and Baker, R. T. (2019). “Evaluating the relationship between clinical assessments of apparent hamstring tightness: a correlational analysis.” International Journal of Sports Physical Therapy, 14(2), 253.
22. Vohralik, S. L., Bowen, A. R., Burns, J., Hiller, C. E., and Nightingale, E. J. (2015). “Reliability and validity of a smartphone app to measure joint range.” American Journal of Physical Medicine and Rehabilitation, 94(4), 325–330.
23. Shipe, N. K., Billek-Sawhney, B., Canter, T. A., Meals, D. J., Nestler, J. M., and Stumpff, J. L. (2013). “The intra-and inter-rater reliability of the tragus wall distance (TWD) measurement in non-pathological participants ages 18–34.” Physiotherapy Theory and Practice, 29(4), 328–334.
24. Werner, B. C., Holzgrefe, R. E., Griffin, J. W., Lyons, M. L., Cosgrove, C. T., Hart, J. M., and Brockmeier, S. F. (2014). “Validation of an innovative method of shoulder range-of-motion measurement using a smartphone clinometer application.” Journal of Shoulder and Elbow Surgery, 23(11), e275–e282.

{kind=link}