Interpreting HRV Trends in Athletes: High Isn’t Always Good and Low Isn’t Always Bad

In this Article
- Why a high HRV score is thought to be good and a low HRV score is thought to be bad
- Why an increasing trend is thought to always be a good thing
- Why interpreting an increasing HRV trend as always a good thing can be misleading
- Why a decreasing trend is always thought to be a bad thing
- Why and when a decreasing HRV trend does not necessarily reflect fatigue
- Conclusion
- References:

Summary
Monitoring heart rate variability (HRV) can provide useful information about training. However, users must avoid using the black-and-white approach that high = good and low = bad. In addition, HRV scores in isolation can be misleading. Any changes in HRV need to be considered in the context of other changes in training, lifestyle, and performance.
Heart rate variability (HRV) monitoring has become increasingly popular in both competitive and recreational sports and training environments due to the development of smartphone apps and other affordable field tools. Though the concept of HRV is relatively simple, its interpretation can be quite complex. As a result, considerable confusion surrounds HRV data interpretation. I believe much of this confusion can be attributed to the overly simplistic guidelines that have been promoted for the casual-end, non-expert user.
In the context of monitoring fatigue or training status in athletes, a common belief is that high HRV is good and low HRV is bad. Or, in terms of observing the overall trend, increasing HRV trends are good, indicative of positive adaptation or increases in fitness. Decreasing trends are bad, indicative of fatigue accumulation or “overtraining” and performance decrements. In this article I address the common notions of both acute and longitudinal trend interpretation, and discuss why and when these interpretations may or may not be appropriate. We will briefly explore where these common interpretations or “rules” have come from within the literature, and then discuss some exceptions to these rules.
This article will mostly focus on the log-transformed root mean square of successive R-R interval differences (lnRMSSD), which is the vagal-HRV index used in popular smartphone apps. For several important reasons lnRMSSD appears to be the preferred HRV parameter for athlete monitoring.
- It can be easily calculated without specialized software
- It is reflective of cardiac-parasympathetic modulation
- It demonstrates greater reliability compared to spectral measures (e.g., HF power)
- It can be assessed in only 60 seconds
- It is less influenced by breathing rate, making it more suitable for field usage
Why a high HRV score is thought to be good and a low HRV score is thought to be bad
HRV-guided endurance training has been shown to be superior to pre-planned endurance training in healthy1,2 and clinical subjects3 for inducing improvements in aerobic fitness variables. Essentially, training with higher intensity/volume when HRV is at or above baseline appears to elicit greater training adaptations. This results in high (or within baseline) HRV being synonymous with “readiness.”
Acute decreases in HRV have been reported to occur following intense endurance training,4 resistance training,5 and competition.6 Therefore, low HRV is commonly thought to provide a reflection of acute fatigue from training or competing.
Where these interpretations can be misleading
Decreased HRV has been observed in a variety of athletes preceding competition as a result of heightened levels of excitement or anxiety.6,7 Further, lower vagal-HRV has been reported to be favorable in sprinters on the day of a race.8
A low HRV score as a result of fatigue also does not necessarily forecast impending reductions in performance. A small case study of 3 high-level tennis players showed that performance markers (VO2 max, single-legged counter-movement jump, and drop jump index) improved following a 30-day overreaching period. The athletes expressed their improved performance at the end of the training program despite showing decreases in RMSSD (between -13 and -49%).9
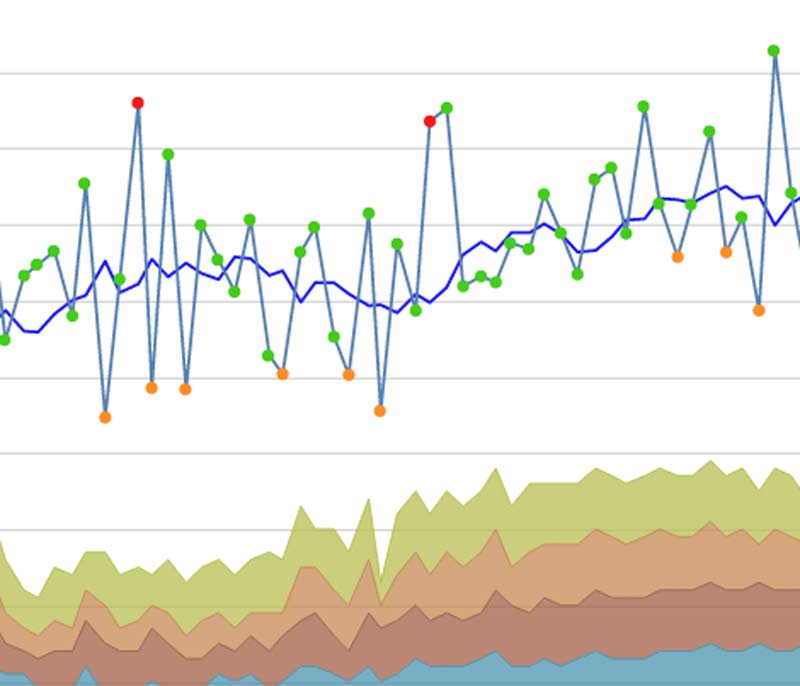
This was also evident in a recent study of ours with a collegiate female soccer team10 that assessed changes in HRV (weekly mean and weekly coefficient of variation [CV, a reflection of the day-to-day fluctuation in HRV scores]) and perceived wellness in response to weeks of varying training load. During a high-load training week, wellness scores and the HRV weekly mean were lower, and the HRV coefficient of variation was higher. All these changes indicate a higher presence of fatigue.
Having devised and implemented the training program, I interacted with and observed the athletes in terms of behavior, body language, etc. They were definitely experiencing fatigue. However, they all completed workouts of higher volume and intensity in both the weight room and during conditioning sessions. This indicates that they were still able to demonstrate their strength and fitness qualities despite fatigue.
Therefore, in the presence of fatigue reflected by HRV, performance may or may not suffer. HRV will typically show changes before performance decrements and thus may serve as an early warning sign of fatigue accumulation. But do not expect your or your athletes’ performance to be poor based on a low HRV score, as this certainly is not always the case.
Why an increasing trend is thought to always be a good thing
Increases in aerobic fitness have often been associated with increases in cardiac-parasympathetic activity in a variety of individual and team sport athletes. A common observation is that those who improve fitness also improve HRV, while those who do not improve fitness show either no change or even decreases. For example, a study by Buchheit and colleagues11 demonstrated that subjects who improved their 10K run time following a training program also showed a progressive increase in their HRV, while non-responders showed no meaningful changes. Large correlations between changes in HRV and maximum aerobic speed and 10K time trials were found.
A recent study of ours currently in press12 evaluated how early changes in HRV relate to eventual changes in intermittent running capacity in team-sport athletes. We found that athletes who demonstrated an increase in their HRV weekly mean and/or a decrease in their weekly HRV CV at the halfway point of a 5-week training program improved performance to a greater extent than those showing the opposite HRV changes. In light of studies like these, interpretation of an increasing HRV trend as being a positive response to training has become popular.
Why interpreting an increasing HRV trend as always a good thing can be misleading
Unfortunately, an increasing HRV trend throughout training is not always a good thing and thus should not always be interpreted as such. In fact, several studies have reported increasing HRV trends in overtrained athletes predominately involved in endurance sports. For example, Le Meurr et al.13 showed decreased maximal incremental exercise performance and increased weekly HRV mean values in elite endurance athletes following a 3-week overload period, compared to a control group who saw no changes. Following a taper, performance supercompensation was observed along with a return of HRV toward baseline.
Why a decreasing trend is always thought to be a bad thing
The most common response to overload training is a progressive decrease in HRV. This is your typical alarm response to a stressor, where the sympathetic arm of the autonomic nervous system is activated. In this situation, resting HR is elevated and HRV decreases. With insufficient recovery time, HRV may not fully recover to baseline before the next training stimulus and thus will result in a downward trend when this cycle is perpetuated. An intense day of training can result in suppressed HRV for up to 72 hours post-exercise.14 With the higher training frequencies and training volumes often associated with overload periods, it makes sense that HRV will show a decreasing trend. Typically, HRV will respond first with a decreasing trend and performance decrements will follow if the overload period is sustained.
A study by Pichot et al.15 provides a good example of a decreasing HRV trend in response to overload training. They showed that middle distance runners saw a progressive downward HRV trend (up to -43%) during a 3-week overload period. In week 4, training loads were reduced and HRV recovered and exceeded baseline values.
Why and when a decreasing HRV trend does not necessarily reflect fatigue
Aerobic exercise tends to have a stimulatory effect on parasympathetic modulation, which can be observed in the HRV score the following morning. This is one reason why moderate aerobic exercise is often used as an effective recovery modality. However, exercise intensity is an important mediator of cardiac-parasympathetic responses to the training session. A recent study by Plews and colleagues4 featuring Olympic-level rowers found that training phases of high intensity (e.g., above the second lactate threshold) suppressed HRV, while phases of lower intensities (e.g., below the lactate threshold) increased HRV.
This is important to understand when interpreting an HRV trend over time. Phases involving moderate intensity aerobic work are likely to cause an increasing HRV trend, while phases of high intensity conditioning with minimal low intensity work will cause a decrease. The absence of low intensity aerobic work results in an absence of the stimulatory effects that this training type has on parasympathetic activity.
Further, the high intensity training will be more disruptive to homeostasis as a result of greater metabolic demand. In this situation, a progressive decrease in HRV can occur despite no meaningful increase in levels of fatigue. Therefore, you shouldn’t be alarmed if you observe a decrease in your HRV trend when limiting moderate aerobic work.
Conclusion
Monitoring HRV cannot be done effectively when following a black-and-white approach to trend interpretation (i.e., high = good, low = bad). Further, relying on an HRV score alone to assess training status will prove to be very difficult. HRV changes must always be taken into context, by keeping track of training load, training type/content, lifestyle factors (sleep quality, nutrition, stress, etc), and performance. These variables are complementary and provide a more complete picture of training status.
Users should therefore observe the HRV trend -> analyze in the context of sport and lifestyle demands (i.e., training load and psychometrics) -> determine the meaning of the change -> adjust training or lifestyle factors if necessary according to the goal of the current phase.
References:
- Kiviniemi, A.M., Hautala, A.J., Kinnunen, H., and Tulppo, M.P. (2007). “Endurance training guided individually by daily heart rate variability measurements.” European Journal of Applied Physiology, 101(6), 743-751.
- Botek, M., McKune, A.J., Krejci, J., Stejskal, P., and Gába, A. (2013). “Change in Performance in Response to Training Load Adjustment Based on Autonomic Activity.” International Journal of Sports Medicine, 35(6), 482-488.
- Behrens, K., Hottenrott, K., Weippert, M., Montanus, H., Kreuzfeld, S., Rieger, A., and Stoll, R. (2014). “Individualization of exercise load control for inpatient cardiac rehabilitation: Development and evaluation of a HRV-based intervention program for patients with ischemic heart failure.” Herz.
- Plews, D.J., Laursen, P.B., Kilding, A.E., and Buchheit, M. (2014). “Heart Rate Variability and Training Intensity Distribution in Elite Rowers.” International Journal of Sports Physiology and Performance.
- Chen, J.L., Yeh, D.P., Lee, J.P., Chen, C.Y., Huang, C.Y., Lee, S.D., and Kuo, C.H. (2011). “Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training.” The Journal of Strength & Conditioning Research, 25(6), 1546-1552.
- Edmonds, R.C., Sinclair, W.H., and Leicht, A.S. (2012). “The effect of weekly training and a game on heart rate variability in elite youth Rugby League players.”
- Morales, J., Garcia, V., García-Massó, X., Salvá, P., Escobar, R., and Busca, B. (2013). “The use of heart rate variability in assessing precompetitive stress in high-standard judo athletes.” Int J Sports Med, 34, 144-151.
- Merati, G., Maggioni, M.A., Invernizzi, P.L., Ciapparelli, C., Agnello, L., Veicsteinas, A., and Castiglioni, P. (2015). “Autonomic modulations of heart rate variability and performances in short-distance elite swimmers. European Journal of Applied Physiology, 115(4), 825-835.
- Thiel, C., Vogt, L., Bürklein, M., Rosenhagen, A., Hübscher, M., and Banzer, W. (2011). “Functional overreaching during preparation training of elite tennis professionals.” Journal of Human Knetics, 28, 79-89.
- Flatt, A.A. and Esco, M.R. “Smartphone-derived heart rate variability and training load in a female soccer team.” International Journal of Sports Physiology and Performance. In press.
- Buchheit, M., Chivot, A., Parouty, J., Mercier, D., Al-Haddad, H., Laursen, P.B., and Ahmaidi, S. (2010). “Monitoring endurance running performance using cardiac parasympathetic function.” European Journal of Applied Physiology, 108(6), 1153-1167.
- Flatt, A.A., and Esco, M.R. “Evaluating individual training adaptation with smartphone derived heart rate variability in a collegiate female soccer team.” J Str Cond Res. In Press.
- Le Meur, Y., Pichon, A., Schaal, K., Schmitt, L., Louis, J., Gueneron, J. and Hausswirth, C. (2013). “Evidence of parasympathetic hyperactivity in functionally overreached athletes.” Med Sci Sports Exerc, 45(11), 2061-71.
- Stanley, J., Peake, J.M., and Buchheit, M. (2013). “Cardiac parasympathetic reactivation following exercise: implications for training prescription.” Sports Medicine, 43(12), 1259-1277.
- Pichot, V., Roche, F., Gaspoz, J. M., Enjolras, F., Antoniadis, A., Minini, P., and Barthelemy, J.C. (2000). “Relation between heart rate variability and training load in middle-distance runners. Medicine and Science in Sports and Exercise. 32(10), 1729-1736.
- Flatt, A.A. and Esco, M.R. (2014). “Endurance performance relates to resting heart rate and its variability: A case study of a collegiate male cross-country athlete.” J Austral Strength Cond. 22:48-52, 2014.

{kind=link}