



My two previous articles on medicine ball training discussed coaching and the science. This third article zooms into the nuances of medicine ball throws and the key factors that transform conventional medicine ball training into the most sophisticated approach today.
Instead of listing common exercises and movements, I’ve taken the most useful information gleaned from all of my mentors and focused on the details that matter. I’ve spent a lot of time visiting great coaches with expertise in speed and power. If you’re looking for the pay dirt on medicine ball throws and want to add more creativity and transfer, this article is for you.


Appreciate the Differences Among Tossing, Throwing, and Other Terminology
You won’t find much in a dictionary or a biomechanics glossary about the differences among the various types of release styles used with medicine balls. Some coaches swap out the terms as if they were synonymous with each other. Eventually we learn the hard way (myself included) that a true difference exists in how we project a ball into time and space.
Even if the science isn’t clear yet, we’re long overdue for a rundown of “what is what” with medicine ball releases. It wasn’t until about ten years ago that I “came to terms with the value of terms” regarding tosses and throws. Like the taxonomy of hops, jumps, and bounds with plyometrics, tossing a medicine ball throw is indeed different than throwing it. And it’s not picky to make a distinction between passing a ball and lobbing a ball. We must use precise language as athletes get hurt every year doing partner work.
While not comprehensive, this group of terms is sufficient to build a better training inventory. I urge you to remember the precise subtleties.
Video 1. Throw. Throws mean just about anything. To be specific, I like to make sure the movement is about releasing the ball over the head or spending the greater portion of the ball’s time above the head generating the force.

Video 2. Toss. A toss usually means the ball is released below the head and generates force from near the knees, often between the legs. The hands often hold the medicine ball in a scoop position underneath the ball.
Video 3. Pass. The pass moves horizontally from the chest. Most passes are not fast as they are square from pressing the ball without using the legs in partnered conditioning.
Video 4. Lob. Like the pass but slower, the lob uses an exaggerated parabolic flight path to help the receiver track and accept the ball with less speed and force. Lob-style exchanges are used often for conditioning or when teaching how to resist the vertical nature of gravity.
Video 5. Put. A put uses a punching action and a single arm release that starts with two hands and either rotate from the legs or twist from the torso. Like the shot put, the action spends absolutely no time generating force above the head. Partnered training puts are simply passed back and forth and employ either a squat-to-put or a transversely created exchange.
This list doesn’t include the actual catch, a valuable part of the movement, and for good reason. Most medicine ball exercises designed for power and explosiveness are about launching the ball. But sometimes absorbing a ball with moderate velocities is beneficial, usually with rotational actions.

General and Specific Transfer with Ballistic Exercises
While the debates over what is general and what is specific may never be won fully, we’ve learned from other concepts that everything has its place. General training may not show up directly with performance, but it has many benefits that help athletes improve systemically.
Specific, or sport-specific work, is very valuable but sometimes has a cost–usually pattern overload or overuse syndromes from performing the same motion over and over. Adding load to a movement that’s done throughout the year looks good in textbooks and workout plans, but they are far from perfect options.
General training can fall victim to the same problems that specific work generates. Pursuing such training milestones as targeted squat numbers or jump distances may not show up on the tape, watch, or film. Specific training may not transfer at all. For example, medicine ball rotational tosses against a wall works the obliques, but so does swinging a baseball bat. Mimicking sporting actions seems like an easy way to improve an athlete because the visual similarities are very close. But the effort usually fails or backfires.
Transfer is the Holy Grail for coaches, but what we pour inside the chalice is just as important. How do general and specific training concepts guide coaches with medicine ball training? It’s actually simple. General training serves a valuable purpose. It challenges the body globally, and it facilitates injury resilience by raising the body’s capacity. Specific work can help boost training rapidly. It’s up to the coach to know when specific training can transfer to better performance and when it’s better to transition to skill rehearsal.
#MedicineBall training conditions the body for general fitness and catalyzes better elastic power, says @spikesonly. Click To TweetIn my experience, medicine ball training conditions the body for general fitness and serves as a catalyst for better elastic power if used correctly. It’s great for warm-ups and for a restorative workout for speed athletes. We can also use it as part of an explosive training program for anyone who wants to maximize their strength and power. High-repetition submaximal throws manage training soreness and heavy training periods. Getting the heart rate up and sweating, however, doesn’t create a neuromuscular adaptation that helps an athlete run faster or jump higher.
At first glance, taking a binary approach to medicine ball training as either maximal power training or general preparation seems too polarized, but it’s a clear and targeted way to communicate to your athlete’s body.

Understand Net Impulse and Summation of Forces
A medicine ball exercise uses the best contribution of muscles and joints to accelerate a ball from a slow speed to a very rapid velocity. And some movements redirect forces back in the opposite direction, usually with partner or ball routines. What’s misunderstood is that sometimes movement patterns are limited to the body’s anatomy, and the release speed will only improve so much because of the athletes’ mechanics.
A chest pass, for example, may not have great speed because the legs are used to stabilize the torso; not involving multiple joint systems likely limits the peak velocity of a throw or toss. Most coaches want to see throws that use as much total joint action as possible to increase the time and distance to generate ball velocity. In theory, faster sports training means faster athletes but as we’ve learned from science, heavy and slow training with fast intent does serve a purpose.

It’s important to understand the value of how forces are generated for two reasons:
- One is to appreciate the locations of the body that may amplify power and those that may leak energy during medicine ball exercises.
- The second is to understand how different techniques or variations may overload muscle groups or even work around injured areas.
Having a full mastery of a small inventory of exercises leads to countless variations ranging from the ability to tweak a movement pattern and enhance a joint system or to rest a muscle group. The most graphic example is a shot put throw–kneeling removes the legs’ contribution and increases the demand on the core muscles.
Manipulating range of motion can help accelerate a #medicineball further after release, says @spikesonly. Click To TweetImpulse is about time and force, and anyone who took high school physics knows that propulsive actions require momentum to be high near the very end of the motion. Manipulating the range of motion can help accelerate a medicine ball further after release.
Throwing for distance or velocity may not be the goal, however. Sometimes having a rhythm that is constant instead of accelerative is important, such as during conditioning exercises and rehab. Keeping the same speed throughout a movement or slowing slightly down can overload areas that are not taxed enough. This is especially helpful for athletes who need more upper body contribution.

Know the Difference Between Hinging and Unfolding
The two actions in medicine ball training–hinging and unfolding the body– are sometimes described interchangeably, but they are two different concepts. For years, I’ve watched different styles and expressions of exercises and wondered why every athlete had their own unique signature and how each interpretation of the major throws and tosses had a unique value. After calling around to some great sprint coaches, I was surprised to learn that many of them programmed what I considered normal variations in technique as ways to reinforce or teach sporting actions.
- Hinge movement and unfolding are two distinct skills that will overlap and occur simultaneously in many sporting actions. Coaches must be aware of the differences and similarities and know when it’s appropriate to introduce or change each movement strategy. Hinge and unfolding movements happen in various degrees with different movement patterns.
- A hinge action occurs when a joint system works mainly in one area or plane. A good example is the Romanian Deadlift (RDL). The conventional RDL hinges at the hip joint. This is easy to see visually because the movement is slow and very simple. More complex activities are starting blocks. While the torso and legs are hinged at the hip, it’s harder to see because of the movement’s speed.
- Unfolding occurs when the body elongates, such as jumping, accelerating, and throwing with the entire body. Most of the time, coaches want yielding (or the body collapsing) and unfolding patterns to enable athletes to accept forces effectively and to produce forces by distributing the strain and propulsion over as many joints as possible.
To use medicine balls effectively, coaches must select wisely among the continuum of hinging and unfolding patterns. Great athletes can do it all, but lesser talents and early learners tend to create patterns that give them the best performance for throw power. Unfortunately, how we create the forces and express them plays a primary role in long-term success and injury rates.
Problems with hinging tend to occur with explosive movements, while unfolding tends to make it difficult to overload beginners who have poor maximal strength.
Consider the difference between an overhead back throw and a granny toss. Both exercises use the body, but the back throw uses more unfolding than the granny toss. Again, most of the time unfolding with the legs and hips is a primary need for sport, but situations exist where primary strain will happen to singular joint systems.

Prescribe Exercises that Have a Specific Purpose
It’s easy to lump exercises into categories that fit visual classifications. Instead select exercises by looking at their role in helping a specific problem an athlete has or meeting the precise need of the day.
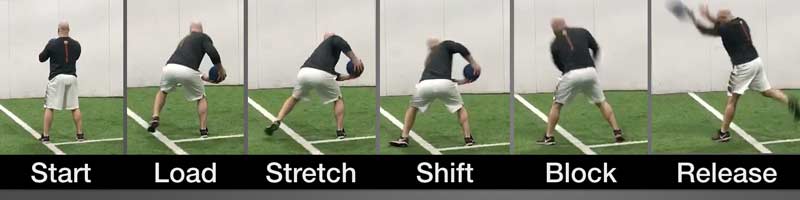
The classic overhead back throw is a good of example of using an exercise for a specific purpose. We see it done all the time by speed and power athletes. You can do the throw with a static start, a counter movement, or a pre-jump, and you can sequence all three to increase demand. Arbitrary placement of exercises, however, is random noise. Coaches can do far better by asking why they are programming an exercise and answering with as much detail as possible.
Another example of a specific purpose exercise is the classic chest-pass-to-sprint exercise, which we see everywhere now on social media. Visually it looks like explosive ballet for speed and power athletes. The question we should ask is: What do we expect specifically from doing this exercise versus another option?
In theory, the 45-degree angle helps increase horizontal forces, especially with a medicine ball. But because an athlete’s power on the first step is highly related to maximal strength, coaches should consider it a temporal exercise. The timing of force application can be just as important as increasing the maximal ability to produce work; chest passes to sprints help teach the paradoxical perception of patience during very fast sporting actions.
Video 6. Everyone loves doing the chest pass throw into a sprint. But for this exercise to create value, it must be better than other options. Some positive benefits exist with this exercise, but remember coaching is about teaching, not just selecting exercises and cues. Video courtesey Brad DeWeese.
Purpose is sometimes confused with transfer. Purpose is about having specific goals that have value beyond making someone better immediately for their sport. Improving coordination is a great investment for training that becomes more intense down the road. Just because an exercise doesn’t get quick results doesn’t mean it’s not valuable. Medicine ball training is analogous to a stem cell, it’s not clear what’s going to grow until later. And the modality has nearly infinite value when the starting point is done right.

Choose the Correct Load Weight for Power and Conditioning
Three load categories exist for medicine ball training.
- Weight that is light enough to throw far and fast is the most common.
- Heavy throws that are not very explosive are used for conditioning circuits or general preparation routines.
- A heavy ball is used as a strength tool, not a throwing option. While limited in application, sometimes it’s useful for specific exercises.
These three categories serve as a simple template for how to prescribe loads for athletes. The eyeball test usually is the deciding factor.


The majority of medicine ball manufacturers incrementally increase the load of their equipment by 1 kg, and typically they range from 1-6 kg. Many coaches, myself included, have pondered whether it matters if a ball is thrown at 3 kg or 4 kg. A small load change won’t dramatically alter the course of an athlete’s career, but the drop in speed and fluidity of motion is enough for coaches to wonder how important load and velocity are for successful training.
- Ballistic Activities: Typically throws have a crisp acceleration without any dead zones slowing the movement. Even when athletes are slightly fatigued, their ballistic actions look fast and efficient.
- Conditioning Activities: These exercises should have the same rhythm and speed from the first repetition to the last repetition. The common thread among conditioning exercises is the summation of forces, or speed stays, rather than constant force. These exercises don’t have that characteristic burst at the end of the throw or pass.
- Strength Activities: Great overload options with very heavy medicine balls should look coordinated and balanced. Coaches want to see a “taming” of the movement, not a struggle. Very few exercises benefit from a heavy medicine ball, but if they’re required, the fluid action must look better than barbells and dumbbells.
Not much room for error exists. It takes experience working with mixed groups of athletes of various abilities. Don’t be tempted to lump exercises in a circuit or routine without adjusting for how the load may interact with the session. What may be perceived as trivial adjustments, such as decreasing reps or increasing distance in partnered activities, will allow for effective training without resorting to constantly adjusting ball loads. Whatever your method, make sure the loads are appropriate and wait to add another kilogram only when the athlete needs it.

Organize Progressions Based on Brain Smarts not Body Strength
Motor learning is very hot right now. We’re currently in the “age of the brain,” and we are deciphering more about how the body and brain communicate and adapt. People think of coaches as a combination of teacher, mentor, leader, and sport scientist. We are burdened with balancing the needs to get athletes more coordinated, more explosive and fit, and more committed emotionally to sport.
Most sports training development programs follow the intensity and volume paradigm. While this is part of the equation for improving an athlete, it’s an incomplete model. Progression is not doing more or going harder, it’s a holistic process designed to help people evolve as athletes.
Classic progression concepts–moving from simple to complex, slow to fast, and easy to hard–are staple principles of coaching. Yet, these ideas fall short of being comprehensive, especially with medicine balls. Many exercises that may appear advanced are actually natural expressions that developing athletes can do early in a training program.
Here’s an example progression with simple overhead back throws.
Squat Throw Option: Static starts with an explosive leg drive are the most common beginner’s exercise because the action is simple and starts without any movement at all. Coaches often use squat throws to prepare for starting power or coming out of the blocks in sprints and hurdles events.
Countermovement Throw: Adding a countermovement or a drop from a standing position increases the demand of the exercise and also the potential velocity. Although most athletes with scant talent can do the exercise well without the precursor squat throw, the progression from static to dynamic actions allows us to see how both qualities–elastic and concentric strength–are trending.
Eccentric Jump Throw: When jumping before the throwing action, an athlete increases the speed of the velocity drive downward and potentially, if explosive and coordinated, the velocity going up and back. Those who have poor differentiation from squats and countermovement style throws should not progress to eccentric jump throws. Instead resources should be spent on fundamental strength qualities.
As you can see, the ball speed increases as does the complexity of the movement sequence. And the amount or demand of the work increases as the exercise order ascends the scale, resulting in a progression of easy to hard. Still, as coaches we can do better than just making things faster, harder, and more complex. Additional ideas for molding coordination techniques are referencing and pairing exercises that are similar. While cues and exercise instruction are the backbone of coaching, tasks that have clear goals usually allow natural movements by tapping into the athlete’s innate abilities that stem from the brain.
From time to time, athletes need to take a step back to take multiple steps forward. Often errors come from a preceding motion–it’s not the action itself that is impaired. Regressions are not necessarily a simpler exercise option; sometimes giving a break from the movement or sequence is the antidote. For regressions, we can load lighter or heavier (to slow things down) and concentrate less on the moving parts, such as only upper or only lower body actions. Alternatively, we can use different types of balls or similar exercises with modifications. This is common with medicine balls that have handles and are excellent options for teaching Olympic lifts and rotational power.
Medicine Ball Power Development Wrap-Up
The list above is both foundational and refined so all coaches can benefit, not just those new to medicine ball training. I’ve seen a lot of beautiful training and testing in my travels, but I’ve also witnessed many of the same mistakes being made over and over with medicine ball workouts. Coaches and sports medicine professionals who want to see relevance and true function will see progress in their outcomes by just applying one of these seven principles. I’ve been lucky to work with great coaches and educated by a few brilliant minds. This information will certainly help the athletes you’re working with.
Since you’re here…
…we have a small favor to ask. More people are reading SimpliFaster than ever, and each week we bring you compelling content from coaches, sport scientists, and physiotherapists who are devoted to building better athletes. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — SF

I enjoyed the parts on how regressions don’t have to mean simple exercises and how these athletes need more general training at times.
Working with mainly middle school and high school baseball players, I find myself keeping my throws sometimes too simple, but I know it’s what they need. For the most part, these kids are playing baseball year round, which means a lot of counter movement and a lot of movements in that transfer and frontal planes. For me, I think that I would be doing a disservice to these athletes by continuing to mimic the movements for baseball. How you explain it I use a lot of the lob throws and for the majority of the off-season training, I have them in a tall kneeling position because I would like to grow them as athletes and eliminate their lower body which they are using year round between throwing and hitting, allowing them to create more force from the trunk.
One thing I wanted to get your opinion on is the use of holds in a medicine ball program. I’ve read a lot about body control and the need to be able to slow your self down. I have started to make my athletes use the same intent they would with the throw but never let go of the ball. Just from watching I have seen an increase in the speed of there throws. of course with this safety is an issue, so I don’t go over 4-6 pounds with my younger athletes. I was wondering if you’ve ever used anything like that before?