

[mashshare]

When I field emails on Electrical Muscle Stimulation (EMS), the most common solutions I share have a back story that is just as important as the protocols. The main uses I have for electrotherapy are for microcirculation and the gray area between rehabilitation and training that I see from time to time. Finally, the age-old problem of dealing with the burdens and strains of frequent travel are also included, making this a comprehensive menu of options for serious athletes. Each “recipe” I share will always include a few important caveats of what may improve outcomes and what may impair effectiveness.
This article is an extension of the earlier piece, “A Guide on Electrical Muscle Stimulation With Athletes,” which gave professionals a foundation to working with e-stim. These six specific protocols should make a noticeable difference that makes the investment in EMS well worth it.
Simple Rules and Guidelines
I don’t like starting off an article with warnings or restrictions, but EMS should not be prescribed without a professional working with someone hands on. No matter how educated an athlete is, or how well-read a coach is, EMS is a tool that overlaps the medical space. Even placing an electrode on the quads for a relaxation setting can be hazardous, and I have seen infections in knee surgery wounds that have opened because someone was a little trigger-happy getting started with rehabilitation.
All of the protocols shared here—even the restoration protocol for managing tone during travel—should be discussed with sports support staff in advance. None of the information and protocols shared replace medical treatment and they should not be construed as medical advice or similar. I believe the corresponding suggestions are the most useful roles for EMS, and I am selective in how I invest my time and money with any modality or method. I have three simple rules when working with EMS and athletes, and they are:
- Athletes should record settings, schedule use, and determine the purpose of EMS when not supervised. My problem with EMS is that it can act like other outside variables, and what is not measured is often improperly managed.
- Do not use EMS for pain management, as it’s a slippery slope and rarely creates a benefit. Let the experts make that choice if they use electrotherapy to manage an injury’s symptoms. For instance, I shared in Part 1 that TENS, a similar treatment, is very shaky in the research as an effective option for pain management. Pain treatment is up to a medical professional and not something coaches or athletes should manage outside of communication.
- Respect the primary mechanisms of training and rehabilitation, and don’t use EMS as a replacement for either. Sometimes something is better than nothing, but EMS is supportive and a secondary option for athletes. It can be convenient to let EMS do the work, as “ice and stim” seems to be the norm with some professionals in sports medicine, but the same thing can be said with coaches who let athletes “zap and go.”
The No. 1 priority with EMS is athlete compliance. Medical TENS feels like it tingles, while performance EMS feels very uncomfortable—this is the reason EMS compliance drops. The six EMS solutions listed below focus on rehabilitation, training, and the restoration of muscular tone.

Post Surgery Setting (Activation)
Right after surgery, the body’s priority is fighting the infection risk, not scoring touchdowns or running at maximal velocity. The use of early EMS should only be initiated after approval by medical staff, as timing is something that only qualified experts should decide. Unfortunately, if you don’t anticipate the opportunity to use EMS before the surgery, you will not likely get any approval if those involved are not already using it. Impact injuries or bone breaks often need a screw inserted, and this makes the use of EMS very limited. Combining metal screws with electricity inside a human body is a potential hazard, so working with the right medical team is necessary.
Post-surgery periods are complicated by the need to resolve pain and the need to get people moving. We’ve shared a good primer on pain science on SimpliFaster, but explaining pain is entirely different than managing pain. EMS is not a tool or method to remove the pharmacology of drug medications or coping techniques; it’s a way to help get the body active immediately after the incision has closed and it’s ready for activity.
In addition to pain, atrophy is another factor that must be minimized. The most obvious is ACL repair, but think about what patterns of atrophy are likely to happen any time a body is cut. Even if the athlete doesn’t go under the knife, any period of immobilization for sport is a complicated process that needs artificial intervention. Obviously, the reduction of size and strength is a problem, but so is the cascade of problems afterward, such as compensation. I will go into this more later with a specific guideline for gait re-education, but getting muscles activated with EMS is a priority.
Muscle contraction in isometric form isn’t going to dramatically change strength and add fitness, but using EMS globally, even with uninjured muscles, is a great start. Besides muscle strength, remember that movement supports the lymphatic system. A combination of pool training (deep water running) and EMS is a great early alternative training option for athletes after surgery or similar.
Solution: Two to four weeks for one to two sessions (no less than 16 treatments) per muscle group daily. Settings can range from low to high frequency, and intensity is what the athlete can tolerate. Duration can range from eight minutes up to active pumping of 3 x 90 minutes per session if the athlete is in a cast or similar. Leave about an hour break between sets and six hours between double sessions.

Gait Assistance Procedure (Locomotion)
I have seen amazing results with an adaptation of the Bill Knowles approach of getting athletes into the water and moving as soon as possible, and getting EMS applied to connect the brain to the injured site and other supportive areas with confidence. Gait analysis is a very broad responsibility, meaning rehabilitation is not consolidated to stimulating a few muscle groups. Nearly any coach can see a visible change in gait, but the subtle differences that are hard to see are usually the problems that become bigger down the road.
The brain and body work together to orchestrate movement, and it’s hard to know when something is central (brain) or more peripheral (limbs). Some professionals attack gait re-education from the feet up, and some from the hips down (most therapists and coaches). A combination of approaches should be used, but ground reaction forces start from the foot and connect all the way to the head. The swing phase and pretension come from the pelvis and brain, so getting stuck with one dogmatic approach is incomplete and painstakingly slow.
Gait training after injury is a profession and more than just part of an article, but one very useful guideline is to use EMS in extreme locations distally and proximally. Areas like the muscles below the knee or the ones more central to the pelvis are the most effective ones to target. Crossover training (training opposite sides or limbs), in addition to unloading options (AlterG and pool), gets people moving normally as function catches up with assistance. Remember that hardware (tissue) and software (higher brain centers) need firmware (nervous system) to be constantly updated with recent successes in training.
Solution: Six to eight weeks for three to four sessions (no less than 16 treatments) per muscle group per week. Settings should be high frequency and high intensity, according to the patient’s tolerance level. Duration can range from eight minutes to 30 minutes, depending on the severity of the injury.
Note: This is not for spinal cord injuries or disease treatment, which both require specialized training beyond typical sports medicine experience.

Foot Strength Package (Function)
One of my favorite studies, which comes from a pressure mapping study done with athletes, is the electromyostimulation or EMS experiment on foot strength and sprinting speed. The researchers learned that, while performance didn’t improve, the forces transmitted through the feet shifted anatomically, giving anyone interested in reducing injuries to specific regions a nice starting point with interventions and analysis. Many coaches have seen the negative results of a barefoot program and other methods of improving foot strength. Now that we have pressure mapping and very good studies on how anatomy, biomechanics, and loading affect joint structures, we are starting to discover why that happens.

EMS and some isolation exercises have value, but they are not going to handle overload as well as a good low load plyometric program. I have outlined side hopping in my plyometric article here. EMS overlays on great conventional programs and is used in conjunction with training and rehabilitation. Combined plyometrics and EMS seem to work great, but most of the studies are not on the foot itself, but on the muscle of the ankle and upward. Electrode placement becomes a bit tricky because it’s hard to target the area, so the standard approach is to just raise the settings high to get as much of the fiber as possible.
Solution: Four to six weeks for two to three sessions (no less than 12 treatments). Use a setting of high frequency and high intensity for 20 minutes per foot.

Maximal Strength Program (Propulsion)
EMS is most commonly used for muscle performance, which is very controversial because most of the studies are limited. The NSCA did a nice job publishing a review of EMS and performance, showing how much interpretation was needed to draw serious conclusions. The article (which has two parts) shared the types of protocols used and the types of changes to muscle performance. I think it is a great review of the literature and can’t say enough good things about the work the authors put in.
Still, they summarized the existing research and many studies as either lacking controls or having a design that satisfies the populations and training that much of us need. Overall, the conclusions were very compelling and the authors stated the following: “The present review shows that EMS training is able to significantly enhance the most important components of the athletes’ performance such as maximal strength and speed strength in the form of explosive movements with maximal forces like, for example, jumping, sprinting, or throwing.”
To be perfectly honest, most of the changes I have seen have been strength changes only. There were a few power improvements and maybe two or three athletes had changes in speed from EMS. I love EMS research, but it’s hard for me to construct my own study. I never want any athlete I work with to be the athlete from the population (control group) that misses out.
Most of the changes I have seen with EMS training have been strength changes only. Share on XIntense muscle stimulation is not really passive. While the volitional element of the contractions is gone from the electrical impulse, the comfort of massage or intermittent compression is also removed. Maximal tolerance is mentally exhausting and it is sometimes at a threshold at which athletes will not comply, or they will reduce the intensity to the point it’s not worth doing. I find that using EMS during maximal phases is the only time I can get sustainable use, as the connection and motivation are there.
I think that one of the reasons Compex created the Mi-Sensor (accessory sensor to manage intensity) was to deliver the right amount of intensity to minimize discomfort, and most coaches believe more is better, at least in theory. I like scheduling the sessions two hours after the actual workout, or using it right before the workout. Having athletes use intense EMS at night has not helped as much and I believe any intense work can interfere with sleep quality.
Solution: Three to six weeks for three sessions (no less than 12 treatments) per week. Use a setting of high frequency and high intensity for 20 minutes per muscle group. I have found is useful on calves, glutes, hamstrings, quads, and sometimes the lower back.

Air Travel Protocol (Circulation)
This protocol isn’t just for air travel; it can be used for prolonged sitting and for bus rides as well. I like using the Marc Pro for travel because it is easy to use, but the PowerDot allows me to leave it on and not have to deal with wires. Many of the athletes I train wear compression when traveling, or they wear very oversized sweatpants to make their legs more accessible while on a plane. The amount of blood flow is trivial, but the threshold needed to make it worthwhile is enough, as athletes notice the difference with stiffness later. While comfort is not recovery, the perceived value is enough that athletes find electrotherapy something they elect to do rather than being told to do.
Video 1: I love using the PowerDot for travel with athletes who want to be road warriors. The video shows a small contraction with the calf that is enough to facilitate the legs but not too demanding that it may fatigue the muscle group.
Circulation is more than just blood flow, as lymphatic kinetics benefit from exercise and stimulate the immune system. Many athletes go too hard on the active recovery side to get an acceleration change in restoration of the body, or they do nothing and get the same result but in different form. Light exercise must be just at the threshold to support the biological internal mechanisms, and not just pile on more strain. Placing electrodes on the calf and getting a cyclical contraction is gold.
Take heed though: If an athlete is not experienced with EMS and does it with too high of an intensity setting for too long, cramping and soreness may happen the next day. I try to use the minimum effective dose by using the lowest visible setting possible and with a slow frequency so the impact is small. I only do this with flights of three hours or longer and always during transoceanic flights or coastal travel.
Other muscle groups are possible but the practical side with the calf is that it’s not considered a risqué muscle area to expose. The travel rules on commercial flights make it a pain to go to the bathroom to take off clothing. I flew in a private jet once and don’t know what teams have for rules, but this is the reason I think the pro teams with their own jets have an advantage.
Solution: Fifteen to 30 minutes for every hour of travel on the lowest intensity and frequency setting that shows visible contraction. I suggest a 2:1 ratio of rest to work.

Body Maintenance System (Diagnostics)
Monitoring the neuromuscular system is nothing new and several discussions on tensiomyography have been already shared earlier in previous articles. As a quick review, EMS is used to stimulate the motor nerves of muscles to produce a contraction that is then measured. Tensiomyography splits the measurements into several characteristics, such as the displacement or stiffness to quantify the tone of the tissue.
Great massage therapists can do this, but unfortunately I can count on one hand the number of soft tissue experts I think can make such a change with tissue at that precision. Using a visual analog scale, professionals can get a traffic light estimation of function. It’s not a perfect replacement for tensiomyography, but it’s a great start for those wanting to be more connected to the specific status of muscle groups.
Self-care with athletes comes with limitations. Self-care is self-administered but not self-prescribed. For every athlete that I have seen succeed with “homework” treatments, I have seen countless others ruined by trying to play at manual therapist. Due to inflamed labrums, laxity issues, and phantom pains from OCD brains, the use of self-care should be handled with caution.
EMS is not a self-diagnostic tool; it provides info to help a professional determine treatment. Share on XA healthy balance of self-care and professional therapy is knowing when to ask for help and when to be independent. Heavy training and competition will leave a body in a state of false alarms and real problems, so interpretation of discomfort and injury is part of the responsibility of both the professional and the athlete. The purpose of EMS is not to self-diagnose but to use it as telemedicine through the communication of the current treatment information to the professional.
Determining muscle diagnostics without a sensor to measure the neuromuscular response is just an estimate, and Compex still does not take advantage of the data they collect after years of me pleading with them to do something. I have emailed and tweeted, and have even been on conference calls with Derek Hansen, but no domestic innovation has yet occurred.
The Mi-Sensor is an accelerometer that uses the motion response to the electrical stimulation to the muscle and sends the data to the Compex controller to deliver an “optimal” dose of current. You can get the Compex Mi-Sensor in Canada and Europe, but not in the U.S. There are several ways to “jailbreak” the data, and I have done it for years, but most of the EMS products don’t export data to the web. The PowerDot does save recent work done on the new app as of late October 2016, and I expect them to open the product up even more in the future.
Video 2: Tensiomyography uses EMS to create an objective response to each superficial muscle tested. While Compex doesn’t provide this type of data to users, a visual analog scale can be done for crude summaries of muscle status with different EMS models.
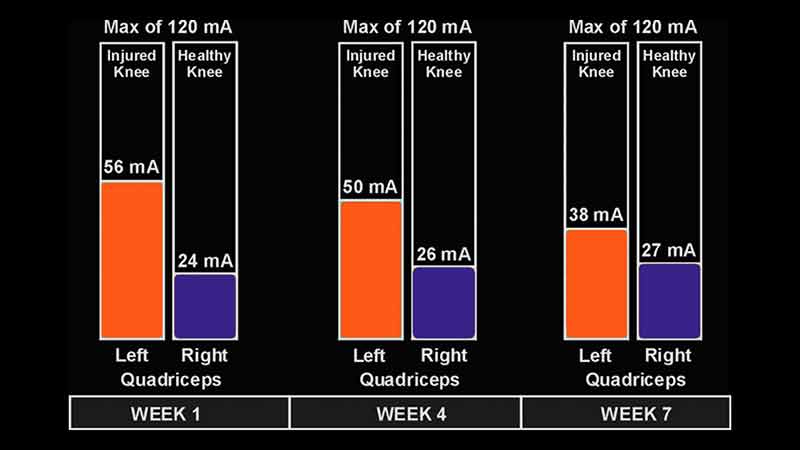
A pragmatic way to see asymmetry and trends is to use my analog technique of looking for maximal contraction and dialing down the intensity until the displacement of the muscle is the same, but the current is minimal to get the same height. This is similar to what Compex does to get the chronaxie, or the time minimum for doubling the membrane excitability of a muscle, and this can give basic symmetry and trends for a season. Investing in tensiomyography isn’t for everyone, and conclusions from this analog approach should be very limited. I have found this to be useful for knee injuries (quad function relationships) and hamstring rehabilitation.
Solution: Constant monitoring before and after games, competition, and heavy training periods. I prefer 48 hours before and 48 hours after for weekly competitions and on off days for other sports that compete more often.
Getting Started With EMS
Several coaches have asked me how to get started with EMS with their athletes, and I always share the simple way to break inertia by using it on yourself. Get a unit and experiment with every setting in order to experience the information and get comfortable using each system. So many options exist. Obviously, I am a fan of the PowerDot, but I do use other devices like Compex and Marc Pro products to supplement our needs.
After years and years of use, the pattern of use typically becomes one of three: You expand the use of EMS over time, you stay the same course, or you use it less and only for special occasions. My first experiments were nearly excessive, and eventually EMS became something that rounded up a comprehensive training or rehabilitation program. Even if you don’t use EMS with your athletes, have at least one e-stim device to stay “current” with what the market is doing. This way, you can be fluent in its use, as some medical programs may require it.
EMS is a practical and supportive solution for better outcomes. A device costing $500-$1,000 is a great investment because it lasts for years, making each use a great bang for your buck. An EMS system should be a tool for the complex or difficult challenges in training and rehabilitation, and integrate the protocols above with professionals in sport if they fit your needs.
Since you’re here…
…we have a small favor to ask. More people are reading SimpliFaster than ever, and each week we bring you compelling content from coaches, sport scientists, and physiotherapists who are devoted to building better athletes. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — SF
[mashshare]



{kind=link}