

[mashshare]
The explosion of interest in electrical muscle stimulation (EMS) from medical professionals and coaches is a great trend. Without education and a careful review of the research though, a good step in the right direction runs the risk of veering off on the wrong path. Over the last few years, I have written about the science of electrotherapy and even listed some protocols that I found to be very useful. I have learned that while adding a complementary modality to a program is useful for rehabilitation, it’s not until it’s really spelled out in the protocols that it becomes widely adopted.
In this article, I cover six emerging trends in EMS for sports rehabilitation, as new techniques are good ways to boost the value of conventional training. When coaches have a strong understanding of both their training program and how adding EMS can benefit an athlete, the convergence is very powerful.
When coaches have a strong understanding of both their training program and how adding EMS can benefit an athlete, the convergence is very powerful, says @SpikesOnly. Share on XBefore I begin, I should mention that the recommendations and techniques are not my own. They are best practices from the therapists and coaches doing complicated rehabilitation of athletes and fixing botched return-to-play programs. When an athlete is injured, it’s usually because the athlete was not prepared to play or that rehabilitation missed an issue that went under the radar. Most of the methods I have recommended before in my articles were passive EMG protocols, basically making sure an athlete added in a session or two of straight vanilla stimulation to their legs or other area of the body every few days.
In no way am I suggesting that you abandon the practice of conventional EMS, though I do know that some more-demanding activities seem to show more promise. My belief is that a passive isometric contraction is very limited, and while EMS doesn’t provide a lot of neuromuscular changes to higher centers, combination methods interact with the brain. It’s not that the modality is a weak signal—it can be necessary noise for improving the outcomes of other approaches.

Whole-Body vs. Single Muscle Approaches
A popular trend in some wellness spas is whole-body electrical muscle stimulation, or WB-EMS for short. It makes sense on paper, as more electrotherapy work done simultaneously looks to be an efficient way to use time and may have some benefit for athletes. I have not seen anything too exciting in the research or found much in practice outside the obvious fact that training variables are a bigger stimulus than the stimulation, it’s a bit of a burden on clinics, and it isn’t team-friendly. I am a huge fan of Kevin Kuske, but I am not sold on the idea that I’m missing out if I don’t use whole-body EMS. I know some soccer clubs use WB-EMS, but I have yet to see any transformation from the practice with athletes.

In terms of the science, WB-EMS isn’t new and has been around for decades. What has changed is the body suit and how it’s sold. Recently, the research has found that aggressive forms of total-body EMS sessions do indeed work, but the real question is how much it works in a real-world setting when athletes are training with a very solid program and conventional EMS or nothing at all. The studies showing potential for WB-EMS are fascinating, but it’s hard to eliminate the exercises from the pure influence of the electrical muscle stimulation.
A WB-EMS soccer study was the most intriguing, but the changes were not dramatic compared to a combined superimposed (read: added but not simultaneous) EMS program that utilizes solid strength training. Whole-body EMS needs to outperform isolated muscle EMS and training, as comparing to a control group isn’t helpful. It’s not that WB-EMS doesn’t work; it just doesn’t work better than great holistic training and regular EMS to a degree worth worrying about.
Video 1. Isometric pulses, or short EMS stimulations paired with static lifts, are a valuable way to get athletes comfortable with intense, prolonged EMS bouts. Early-stage rehab using isometrics and EMS is a great option for athletes.
Functional EMS, or basically any training program that looks like training on one’s feet (read: active), works, even with isolated stimulation to one area or muscle. A few years ago, a study on lower extremity (below the knee) EMS and sprinting was very promising for improving sprinting speed in just three weeks, and my own experiments saw very similar results. I was surprised, as I was convinced EMS wouldn’t help sprinters, but it may be needed for team sport where opportunities for training and recovery are low.
Personally, I see EMS and lower body work as fine after injury for sprint athletes or for team sports during off-seasons. Usually, anything I repeat from the studies washes away because of confounding variables or advanced populations, but this protocol worked very well. It’s not that total-body or whole-body EMS is a waste of time, it’s just one option that may not prove to be as exciting as it looks in marketing videos.

Combining Electromyography and Electrical Muscle Stimulation
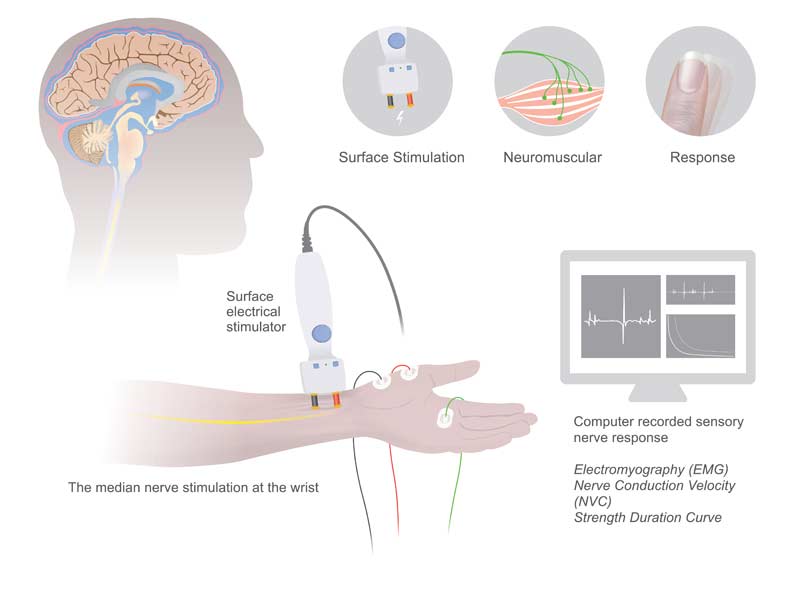
Nerve conduction velocity (NCV) testing is a grey area in performance, as nearly all of the use is for injuries, not optimizing athletic success. Fortunately, the sports medicine side is aware of what happens when nerves are damaged or impaired, and an NCV leveraging electromyography is useful for addressing those concerns. Interesting research on symptomatic and asymptomatic spines with medical imaging (MRI) and electrical diagnostic testing (nerve testing) hinted that if you want better status of function, it’s more effective to use a combination of tests than just one alone.
We’ve all likely heard the joke that MRI means “might reveal injury,” but it’s more about how to use imaging correctly than seeing it as a waste of time and money. You don’t use a nerve conduction velocity test for pain; you use it for function of the neuromuscular system as a way to see impairment, usually coming from a disc pathology or similar. I recommend exploring the use of biofeedback of EMS and electromyography as a way to help athletes improve their early stage rehabilitation, especially after major reconstructive surgeries or times where they are really beat up and unable to train normally.
A good example of EMS and EMG pairings stems from my observation of a few athletes using functional electromedicine. Managing compensations to the shoulder joint after labral repair and with teaching athletes to walk and sprint after surgery is a challenging endeavor. I also see benefits for athletes who have poor speed and local atrophy of muscles from impact injuries—usually peripheral nerve injuries. I am not a sports medicine professional, but after listening to a few progressive and very successful specialists, I am now more interested in muscle function with electromyography than I was before.
Instead of handing out painkillers, I think we need more evaluation of the impacts to the nerves themselves. In any case, testing matters and using EMG right after EMS application can help both the clinician and athletes see meaningful progress. Of course, outcomes are about real-world movement and performance, but early stage work that isn’t racing the clock (as much) should use a combination of muscle stimulation and muscle activation measurements.

Eccentric Training and EMS Treatments
Coaches have been experimenting with combined resistance training and EMS for years, but most of the efforts have been isometric pairings. Isometric training with stimulation makes sense, as a prolonged contraction from electrical current is similar to an isometric contraction from specific exercises. When EMS is used during the training of concentric or eccentric motions, especially multi-joint actions, it becomes very complicated due to the duration of the current and the timing of the movements. Squatting slow with EMS on the quads eccentrically is different than rebound jumping, so combined methods are not easy to administer. Wireless EMS improves the ability to use exercises of choice, but traditional wired devices are still very useful in rehab settings.
Video 2. Slow eccentric tempos are good for those that are progressing towards true overload options. External stimulation with functional movement (ground-based strength training) is a strange experience and must be delivered carefully.
I use EMS with athletes for several reasons, but the most important reason is to override the fear of effort or pain. When an athlete is hurt, they may believe their muscle will reinjure or that they will be in pain from the previous injury. This is typical and very normal. I am not a physical therapist, but if you do any reconditioning after injury you will still need to manage lingering discomfort or strange soreness. An athlete often guards an injury and a muscle will fire early to prepare to support a joint, fire late because it’s inhibited, or fire too low. I have yet to see a muscle fire with more effort than the other limb, but I don’t have a lot of experience using EMG in rehab except for some very complicated cases.
I use EMS with athletes for several reasons—the most important reason is to override the fear of effort or pain after injury, says @SpikesOnly. Share on XEccentric training is not just about structural changes or endocrine responses—it’s a true natural boosting agent to the brain. With EMS bypassing the CNS, does combined superimposed training cause a problem? I don’t think so, but I am curious to only use EMS with movements that I know the athlete can control with a high degree of coordination.
Research on cortical excitability with EMS is available and difficult to decipher, but we can’t be all or nothing anymore with theory. I don’t see much information on ballistic or explosive functional electrical muscle stimulation; just a lot of isometric or brain disease use cases. You can argue that EMS implemented separately is just as effective, and I might agree, but those athletes who don’t seem to trust the process or themselves respond extremely well, and the force analysis and muscle activity readings support the findings. I don’t know if it’s a parlor trick (placebo) or a unique contraction, but functional EMS doesn’t need to resort to split squats and long durations anymore.

Blood Flow Restriction and Muscle Stimulation
A strange but growing trend is the simultaneous use of EMS and BFR (blood flow restriction), and some therapists and experimental coaches use both methods in various sequences or progressions. I don’t have any experience that can shed light on the ideal protocols, but I have observed the daily grind of rehab and know that athletes respond better than without the modalities. I wrote about BFR earlier and was sure to explain that occlusion-type training helps with local or peripheral adaptations. The same argument can be made for EMS, where athletes are not adding a lot of neurological adaptations to the body by simply sitting in a chair watching Netflix and receiving stimulation treatment.
Challenge injured athletes before they go to surgery. If an athlete is having an elective procedure, do everything possible to prepare them for the rehab, says @SpikesOnly. Share on XSo why double down on two modes that are not enriching the nervous system much? Well, the answer is simple: You need to challenge athletes who are injured before they go to surgery, not only right after. Athletes often go straight into surgery after injury so not much can be done, but if an athlete is having an elective procedure weeks out, I recommend doing everything possible to prepare them for the rehabilitation.

Coaches are getting great results from the combination of active BFR sessions with passive EMS treatments, but what about using the two modalities at the same time? At first, I thought it was silly because it looked a little odd, but scientifically I did foreshadow this in the SimpliFaster article referenced above. Most of what we know comes from animal models, so this is very early, but combined methods may be a good alternative when options are scarce.
A study that’s nearly a decade old measured serum growth hormone after a combined session of BFR and EMS, but we need to remember growth hormone response and actual growth hormone action are not the same thing. You can starve rats and growth hormone levels will rise, but that doesn’t mean an athlete will start improving their strength and power. A later research study on recreational athletes repeated the concept of using electrical current and blood flow restriction training and found it increased isometric strength of the legs. Ideally, more studies on athletes and with dynamic and explosive movement would be nice to see, but it’s going to be up to the pioneers to see what truly can be done with this approach.
Based on the little research available and the complications with mixing methods, I am still very cautious about recommending this approach outside of one-on-one environments. While group BFR sessions are trending in California, I am not a fan of mass rehabilitation, by any means. Feel free to experiment with EMS and BFR, as several therapists are treating diabetes patients and other populations with the same technique. The question is the magnitude of change and what circumstances an athlete is in. I don’t know if this method is great for plateaus or only appropriate for early rehabilitation. Shoulder, knee, and ankle return to play is exciting to me, as I have seen impressive changes quickly with the approach, but more research is needed to figure out how far we can take a stacked method.

PNF Stretching, Potentiation, and Recovery
Manual therapists, who do most of the work during a therapy process, can benefit from adding EMS-assisted therapy with PNF (proprioceptive neuromuscular facilitation) stretching. During heavy training, an athlete’s tightness is due to a combination of peripheral contracture and neuromuscular guarding. If a therapist or even a solo athlete with an Exer-Genie uses PNF, the addition of muscle stimulation may work. I am not sure if reciprocal inhibition is the theoretical explanation as there is some conflicting research with PNF, but I do know it works. What makes it challenging is the protocol of having an athlete receive therapy that is active and assisted while receiving a series of EMS treatments. Therapists can work with the rhythm of the settings or customize it with the athlete controlling the stimulator.
PNF stretching can help reduce a cramp but it likely won’t prevent one. Cramping can be induced by electrical stimulation purposely for scientific studies, but we do know the combination of PNF and EMS works, and support exists. Most of what I have seen with speed and power athletes comes from some coaches who do their passive potentiation work in combination with PNF and EMS. This is a very grey area, as EMS alone doesn’t have the potency that I see with actual training, but then again PNF is not just stretching per se. PNF is active muscle contractions, so I do see it used when speed athletes want to feel open but not tired.
Often athletes who are incomplete with their rehab need a quick fix—something I don’t like but must accept when sport rewards availability. I am no fan of athletes competing short or injured, but this is going to happen whether we like it or not. We can use PNF as a combination of diagnostic (with load cell) of readiness and restoration of range of motion to ensure past injuries don’t cause new ones. It’s hard to guess where late return to play truly ends, but using EMS and PNF can help us see trends in the process, which is something Derek Hansen has advocated for years.
Video 3. PNF is a lost art, and simple therapies with EMS work well in the clinical setting. Additional current and measurement technologies improve outcomes and add confidence in the return-to-play program.
A very common question coaches have is the timing of PNF stretching during the day, as some coaches fear that stimulation may interfere with sleep. Just as coaches worry about static stretching before speed and power, they worry about the opposite when they want their athletes to rest and relax. A lot of coaches use light stretching before bedtime, and I frankly don’t see the need to add EMS to evening routines. On paper it may not be an issue, but why take the risk?
I frankly don’t see the need to add #EMS to evening routines. On paper it may not be an issue, but why take the risk? asks @SpikesOnly. Share on XSome therapists instruct athletes to receive EMS for about 20 minutes before their training session, and claim it works wonders later. So far, I have only seen acute spasms benefit from EMS, and all the athlete has to do is be prone or supine for an extended period of time.

Readiness to Train
The last area that is emerging as a potentially valuable one for coaches is tracking the current settings intelligently as a way to learn an athlete’s ability for recovery and to rehabilitate them. So coaches don’t think EMS means prediction or fatigue monitoring, readiness of electrical current logging is more about a qualitative response to tissue, even if the precision of the discharge of current is accurate or known. The limitation of electrode placement repeatability and the analog estimation of tissue response is why the process of working with EMS is more about the experience than the equipment.
Several companies have attempted to provide either a shortcut for delivering stimulation or training to help professionals estimate this, but they are not the same as tensiomyography readings. With tensiomyography, the sensor actually measures tissue responses versus visually seeing contractions or detecting a contraction.

Compex has provided its MiSensor for years—it’s basically an accelerometer and an algorithm to adjust the current based on the muscle response. Their patent covers the time after delivery of the current to contraction phase to estimate the chronaxie of the muscle. Bioelectric currents operate with the notion of thresholds: how much current is needed to create a physiological response. The Compex company believes that by identifying those thresholds, it can automatically detect the ideal setting of current to deliver the optimal electrical stimulation. In their patent, they offer the following explanation:
[The] control system, in communication with the sensor system and accelerometer device, determines a muscle chronaxia during a measurement phase of about one to several seconds. This measurement phase comprises applying several different pulse durations to the target muscle in order to determine points of the curve…. By mathematical curve fitting, the value of chronaxia can be determined. This function is preferably implemented at the start of the program by a short sequence during which measurements are taken. Once the test has been completed, the primary stimulation program can start.
Theoretically, they are using a calculation from a century ago to automatically provide a setting for individuals, bypassing clinical experience and alternative approaches that see a big picture rather than a local response from a single input. I love the technology and understand that “zapping current” 4-6 times the rheobase could cause tissue damage with engineered models. We can expand on this methodology, as muscle is a complex organ system.
So what is the takeaway? Most coaches and therapists want something tangible to use during their next treatment time, so I will cut to the chase. A muscle functions better when it is consistently excitable, and that means the tissue is responsive and fast. Logging current and its response to training is not a direct measure of fatigue or readiness, but it does have a strong relationship to function when merged with other data points, such as direct performance tests like the RSI (reactive strength index) of hops and actual speed tests. The details of how to apply this method are beyond a blog or article, but learning more about muscle neurophysiology and training is a wise investment for return-to-play strategies.
Tweak and Experiment with Sound Reasoning
I don’t want to sound preachy, but EMS is about years of commitment—not just a few sessions. If you want to get the most out of the modality, you can’t just try it for a few weeks and expect much to occur, even if the research shows a small benefit. The addition of EMS will not turn a donkey into a racehorse, but it will help you make strides in complex injuries and very difficult performance problems.
The addition of EMS will not turn a donkey into a racehorse, but it will help you make strides in complex injuries and very difficult performance problems, says @SpikesOnly. Share on XI have tried all of the techniques above and added them to my toolbox, and I want to ensure your war chest is full as well. You may never or rarely use an EMS technique, but knowing how the protocols work helps with your everyday training. The challenge of integrating EMS is not just with the waveform or current settings; it’s really about troubleshooting real-life problems. This article can help you get your athletes back on the field better than they were before, but only if you make an effort beyond what most professionals are willing to put in.
Since you’re here…
…we have a small favor to ask. More people are reading SimpliFaster than ever, and each week we bring you compelling content from coaches, sport scientists, and physiotherapists who are devoted to building better athletes. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — SF
[mashshare]


{kind=link}