Direction Bias Gym Programming and Athletic Performance

In this Article
- What Is Direction Bias?
- The Use of Clinical Pilates in the Athletic Population
- Introducing Direction Bias Gym Programming
- Hypothesis for Direction Bias Effect: Central Pattern Generators
- The Potential Benefits of a DB Gym Program
- Post-Hoc Analysis of the DB Group
- Does This Mean We Only Focus on the Flexion-Biased Athletes?
- Further Research
- Summary
- References

Summary
Direction Bias programming is the evolution of the validated concept of Direction Preference, which has demonstrated that repeated movement in an individual’s preferred movement pattern yields improved function. Preliminary DB studies show that certain heavy resistance exercises, when matched to the individual, can lead to improved athletic performance.
What Is Direction Bias?
“Direction bias” is a term derived by Craig Phillips, who developed the treatment method of “Clinical Pilates” more than 25 years ago, when he created the Dance Medicine Australia (DMA) method of Clinical Pilates courses in Australia. Since that time, over 10,000 physiotherapists have taken the courses worldwide. These courses expand on Joseph Pilates’ original Pilates method by emphasizing the prescription of a specific exercise to match an individual’s direction bias (DB).
Direction bias stems from “direction preference,” which is a validated assessment tool1 used by McKenzie-trained clinicians. With it, a subject’s symptoms and/or mobility improve with repeated movement in one direction and worsen with movement in the opposite direction. By using direction preference to guide exercise prescription in patients with chronic lower back pain, outcomes improved by up to 780%.2
The assessment of DB occurs through observation of a subject’s movement quality in a three-part battery of standardized dynamic stability tests following the same repeated direction-specific exercises. According to research, the tests are highly reliable,3 allowing for the assessment of DB in the asymptomatic individual, and opening up its use in the athletic population.
For more information on the technique of direction bias assessment, I recommend the article by Tulloch and Phillips,4 as well as these DMA Clinical Pilates courses.
The Use of Clinical Pilates in the Athletic Population
Pilates, while normally synonymous with rehabilitation, has been utilized in the field of high performance for over a decade, but to date there is only anecdotal evidence supporting its performance benefits. Similarly, although programs at English and Australian institutes of sport have used Clinical Pilates (CP) extensively, there are no long-term quantitative studies published on its benefits.
In an unpublished 2014 study,5 I found that in an untrained population, both traditional Pilates and CP improved repeated vertical hopping performance on the participant’s non-dominant side after six weeks. However, among trained athletes, it was only Clinical Pilates that yielded a significant benefit. Furthermore, Turner demonstrated a 6% improvement in rowers’ ergometer power results following the addition of Clinical Pilates intervention to their training.6
Acutely, Tulloch and Phillips showed a “within-session” 14% vertical hopping difference between prescribing “matched” and “un-matched” CP exercises to the participant’s DB in an untrained population.4
So why the resistance to using Pilates as part of strength programming at the elite level?
Conversations with numerous national level coaches across a wide variety of sports point to the low-load, controlled focus of Pilates as a poor match for the strength and power demands of many elite sports. I recall one such strength coach at a NRL Rugby League team saying to me, “If you put a reformer in this gym, I’ll throw it through the window followed by you.”
Furthermore, the focus of controlled movement and breathing in Pilates is often not synonymous with the intensity of effort associated with many athletes’ and coaches’ perceptions of training requirements at the elite level.
However, Figure 1 demonstrates that injury rates are increasing…
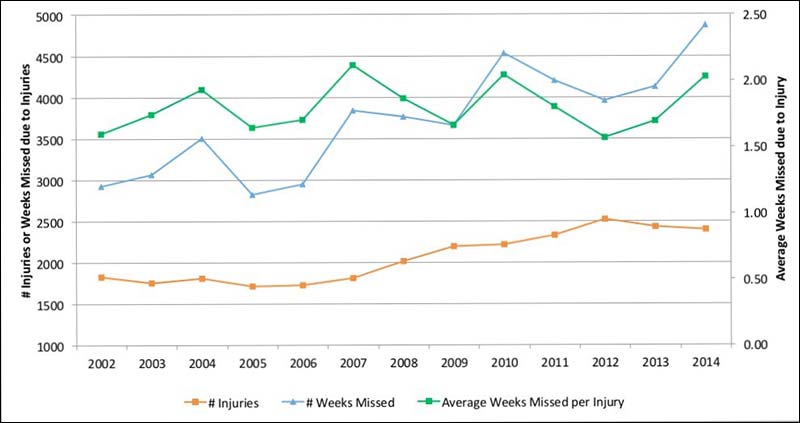
We need to focus on more than just strength training for injury prevention (Dan Pfaff)
The traditional belief that you can bulletproof an athlete through resistance training alone is being refuted. Local joint and tissue training strategies are not enough. Coaching methods now view training at the central nervous system level (CNS) as necessary to engage sensorimotor control through neuromodulation and sensory stimulation.
Introducing Direction Bias Gym Programming
DB gym programming prescribes the appropriate exercise to the athlete according to how they respond to repeated movement either towards or against their individual DB, using heavy resistance exercise.
Athletic training is the study of stimulus and outcome, where CNS regulates the outcome. While there are examples of the over-riding effect of descending cortical input on movement patterns, the CNS will primarily try to keep the host free from harm, particularly when loading.
One of my favorite quotes is: “The body is only as strong as it feels safe,” by Perry Nickelston. If the CNS determines that there is a potential threat to itself, it will restrict and/or alter movement patterns.

Inappropriate exercise selection has shown that regardless of the conscious cueing and training involved, some movement patterns will either not improve or will deteriorate, particularly under load. Conversely, with minimal coaching, the correct exercise selection can repeatedly demonstrate improved movement patterns that immediately carry over to other functional tests. The answer to this phenomenon lies in the hypothesized mechanism for the DB effect.
Hypothesis for Direction Bias Effect: Central Pattern Generators
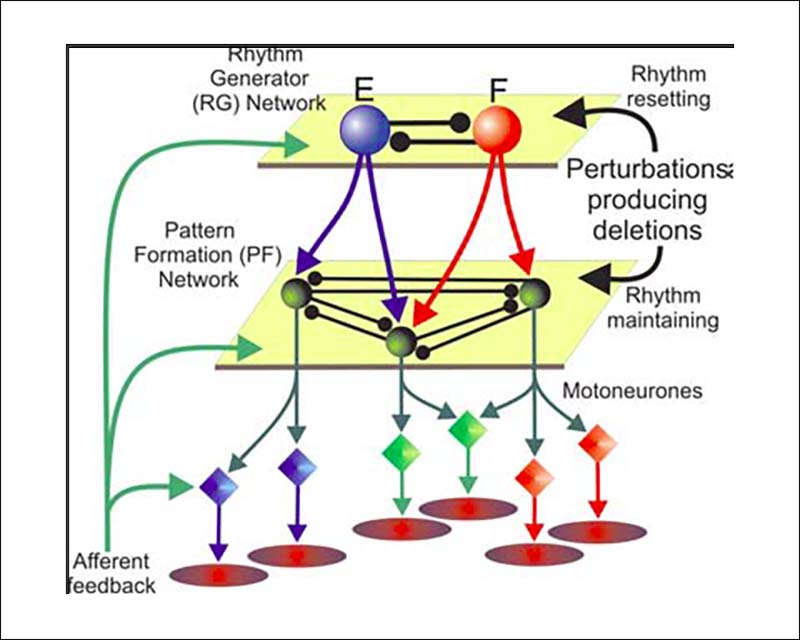
Central pattern generators (CPGs) are networks of nerve cells that produce rhythmic, specific movements without conscious effort. Each joint, bilaterally, may have its own CPG that it communicates with via intermediate neural circuits.7
Theoretically, the CPG consists of two sections, the rhythm generator (RG) network and the pattern formation (PF) network, before providing excitation of multiple synergistic motor neuron pools responsible for different phases of movement. Each of these levels is subject to afferent feedback that can alter the level of motor neuron activation, timing of the phase transitions, and/or frequency of the impulse.
By this means, there is a hypothesis that pathology may disrupt the signal intensity at the RG level and/or the pattern of firing of either the extensor or flexor group at the PF level. This results in reduced quality of movement by diminished motor neuron firing, and therefore altered motor patterns.7
Potentially, DB exercise acts to negate the modulating effect of the pathology through its preferential stimulus to either the inhibited flexor or extensor pattern, providing positive afferent stimuli to restore the original CPG. Furthermore, spinal position can facilitate and inhibit CPGs,8 suggesting that exercises moving into extension will preferentially excite the extensor pattern at CPG level. Clinically, this is supported by the immediate effect of DB exercise intervention seen on brainstem-injured patients, where extension exercises tend to improve patients with acute brain injury, overriding the frequently observed flexor spasticity pattern.
For more information, I invite the reader to read the excellent article by Rybak.7
So how do we know which exercise has which Direction Bias?
The direction bias of an exercise can be theoretically categorized as:
- The position maintained by the lumbar spine at the “sticking point.”
- The predominant movement at the lumbo-pelvic-hip complex.
- Counter torque required against COG.
However, due to the complex multi-segment movement of many resistance exercises, classification is far from simple. A research study proposed for 2018 will compare the acute effects on dynamic stability and athletic performance of four common heavy resistance exercises: the dead lift, back squat, front squat, and recline leg press.
So far, case series data has been collected across seven athletes. The objective measure was the flight time/contact time ratio for the athlete over five repeated vertical hops when told to jump as high as they could with minimal contact time on the ground.
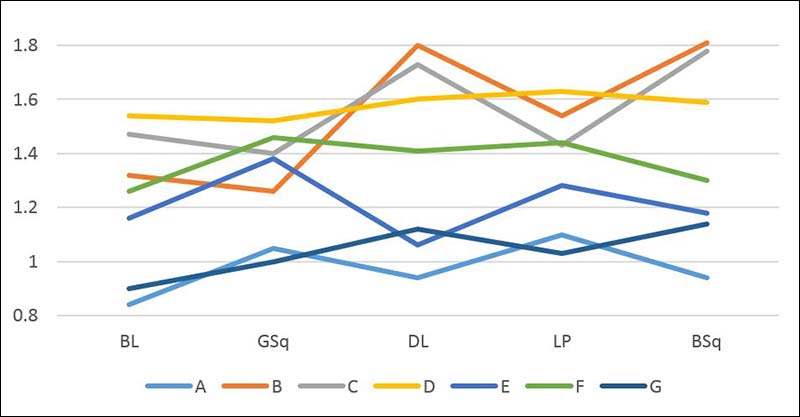
The results for Athletes A-G are not significant for acute change on repeated vertical hopping performance before post-hoc analysis. However, prior to the four resistance exercises, each of the athletes was tested for their DB and the results are as follows:
This demonstrated the acute performance improvement seen with a “matched” versus “unmatched” Clinical Pilates exercise on vertical hopping performance, consistent with the results of Tulloch.4
Therefore, when results are analyzed, the resistance exercises classify as follows:
- Extension – Dead Lift and Back Squat
- Flexion – Front/Goblet Squat and Recline Leg Press
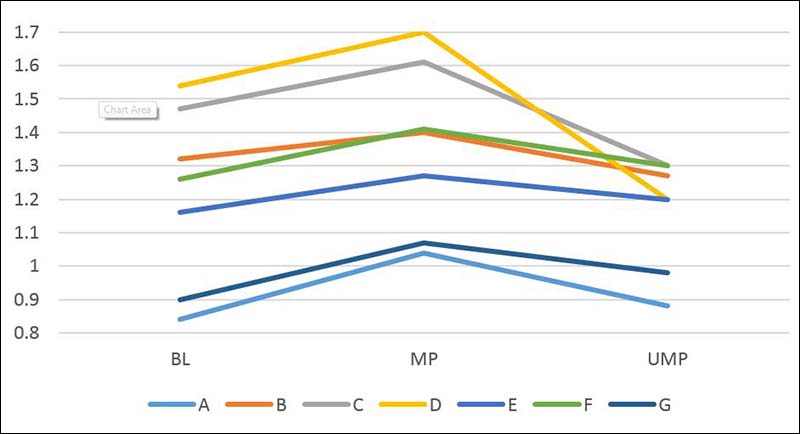
Below is the redrawn graph showing the results for each athlete’s performance respective to whether the resistance exercise was “matched” (MR) or “unmatched” (UMR) according to their direction bias and the bias ascribed above.
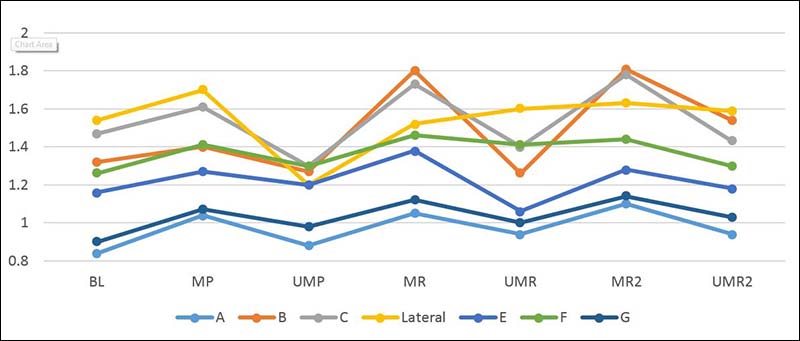
This preliminary case series supports the hypothesis that resistance gym exercises with a DB can behave in a similar way to low-load Clinical Pilates exercises.
One of the athletes in this analysis did not respond in a predictive manner like the others. Follow-up testing revealed that this athlete had a “lateral bias,” meaning he did not respond to flexion or extension movement like the other athletes, but responded better to a lateral movement. As the gym exercises chosen were bilateral frontal plane in nature, there was minimal response to the stimulus of the “lateral” athlete. This needs to be a consideration in DB exercise prescription and it warrants further study.
The Potential Benefits of a DB Gym Program
Obviously, there are many more exercises than these four that make up a program, and many more will require further classification to become a useful tool for both clinical and performance parameter decision-making in the gym. However, using the three questions outlined earlier on how to theoretically classify the DB of an exercise, we can provide an “educated guess” on the classification of certain exercises.

I presented a pilot study at the 2015 SMA National Conference, considering the effects of an eight-week DB strength program.9
The study consisted of 43 athletes allocated to either a DB group (n=25) or a “mixed” (non-DB) group (n=18). DB group athletes received a program that consisted of bias exercises “matched” to their individually assessed DB (e.g., athletes assessed as having a flexion DB participated in the Flexion Bias program). Of the 25 athletes, there were eight with flexion bias and 17 with extension. Mixed Bias program athletes participated in a mixture of both DB programs, which acted as a control for this study.
Sixteen exercises were theoretically classified as either Flexion or Extension as follows:
| Flexion Bias Exercise | Extension Bias Exercise | Mixed Bias Program |
| Front Squat | Back Squat | Front Squat |
| Recline Leg Press | Dead Lift | Dead Lift |
| Pistol Squat | Bulgarian Single Leg Squat | Pistol Squat |
| Forward Lunge | Backward Lunge | Backward Lunge |
| Seated Knee Extension | Kneeling Overhead Press | Seated Knee extension |
| Seated Calf Raise | Triple Extension Calf Raise | Triple Extension Calf Raise |
| High Step Ups | Step Downs | High Step Ups |
| Romanian Dead Lift | Loaded Carry | Loaded Carry |
Athletes performed a total of 20 sessions of this program over eight weeks, with testing at four and eight weeks. The following results outline the percentage change from baseline after eight weeks of intervention.
| 6 Vertical repeated Hop (Bias side) | 6 Vertical repeated Hop (Non-Bias side) | 3 Hop for maximal distance (Bias side) | 3 Hop for maximal distance (Non-Bias side) | Agility (5-10-5m shuttle) | 20m Sprint | |
| Control | -0.9% | -3.5% | 3.6% | 6.1% | 2.5% | 2.1% |
| DB Group | 14.4%* | 18.1%* | 10.9% | 10.5% | 7.0%* | 2.6% |
In summary, the DB group responded better across all measures compared to the control standard intervention. In particular, repeated vertical hopping and agility testing between groups saw statistically significant effects.
Though not significant, 20m sprint times reported similar results to Brown et al.,10 following unilateral direction-specific (posterior chain) focused exercise protocol where there was no control group.
Post-Hoc Analysis of the DB Group
Practitioners familiar with DB are aware of the higher concentration of flexion-biased athletes at the elite level compared to the sedentary population, as well as the difficulty in prescribing loaded exercise to a subgroup that traditionally resists compression/extension. Unfortunately, due to the paucity of research in DB, this is not well-known across the worldwide high-performance population.
However, these athletes are commonly the ones that display many of the following characteristics:
- Excellent flexibility/mobility
- Soreness with repeated gym sessions, often requiring significantly longer breaks between sessions than their compatriots
- Extreme levels of “natural” ability
- Frequent injuries
I am sure many of you reading this are thinking, “Yep, I know athletes like that.” These are typically “flexion-biased athletes,” and I think traditional compressive resistance exercises are prone to endanger this group.
Post-hoc analysis of the above study revealed the following startling chart.
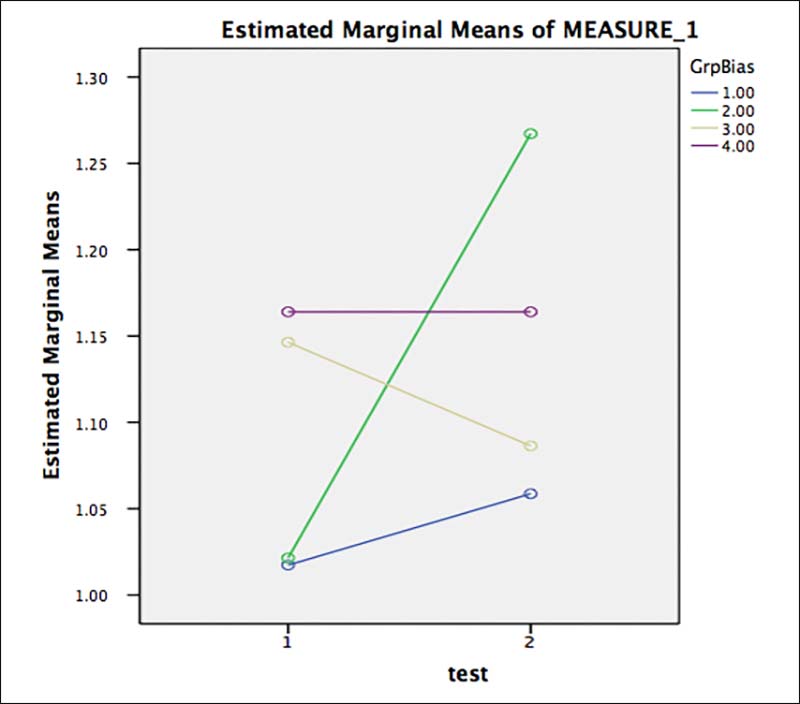
In this chart, the green line represents the Flexion group of the DB group, the blue line the extension DB group, the beige line the Flexion Control group, and the purple line is the Extension control group for the repeated six vertical hop tests.
The summary of this data is highly suggestive that traditional programming does not account for DB (control group) for vertical hop performance. It can be shown to be detrimental for flexion-biased athletes, and is equivocal for extension. However, with implementation of the DB program, extension-biased athletes improve significantly and flexion athletes improve off the scale!
This sub-group of athletes will be the subject of further research due to their natural performance attributes—and, hence, value to the team—as well as their history of predisposition to injury. It’s certainly something worth investigating for your athletes.
Does This Mean We Only Focus on the Flexion-Biased Athletes?
There are certainly a sub-group of athletes that respond better to DB exercises than others. I often refer to these as the “Responders.” These are the ones that demonstrate a large performance improvement after a matched exercise but, conversely, a large degradation in performance with an unmatched DB exercise. As a result, care needs to be taken with their programming. As outlined above, flexion athletes often fall into this category, as do the acutely injured.
Those that respond least tend to be more robust and can tolerate exercises across both flexion and extension movement planes—we refer to these as the “Robust.” These athletes will still have a DB of some degree that is potentially worth considering at least for heavy loads, new techniques, or the novice lifter. Raysmith and Drew found that if an athlete can complete more than 80% of planned training sessions, there is a 700% increased likelihood of them reaching their performance goals.11 Therefore, performance improvements may be associated with DB gym programming because of the potential to protect the athlete by restricting possibly injurious exercises.
As with everything, there is a spectrum at play here, and the point at which the coaching team decides that an athlete’s classification should be a “Robust” versus a “Responder” is an area that requires more research. The net worth of a “Robust” athlete on the far end of that spectrum, undertaking a DB program compared to a compound multi-plane movement focus, is likely low. Suffice to say that this emerging area of performance training will highlight the need for communication between performance staff and physiotherapists trained in DB assessment.
Further Research
The long-term goal of the coaching team, in addition to performance enhancement, is injury prevention. It is well-recognized that the team that keeps its best players on the field for longer has the greatest success.12 DB programming has the potential to identify and turn a “Responder” into a “Robust” through exercises prescribed to facilitate the CNS’s control. As the athlete progresses, measuring their tolerance to loading into their “opposite” DB (through un-matched exercises) compared to their matched exercise response will generate a picture as to their current training state. There is a planned 12-month follow-up study of injury incidence for the athletes in the pilot study.
Summary
DB programming is the evolution of the validated concept of Direction Preference, which has demonstrated that repeated movement in an individual’s preferred movement pattern yields improved function. Preliminary studies show that certain heavy resistance exercises, when matched to the individual, can lead to an acute performance effect, and when not matched, a degradation.
By incorporating these “matched” exercises into a specific program for the athlete, there were significant improvements over traditional “mixed” programming in single leg power and agility testing. Further analysis demonstrated that certain subgroups may be more susceptible to DB than others, highlighting the need for their early identification by performance staff, as acute exercise selection may lead to potential performance gains, as well as improvement through reduced risk of injury.
DB programming has great potential in the field of high performance sport, but more research is necessary for its validation and widespread use.
References
- Edmond et al. (2014).
- Long et al. (2008).
- Yu et al. (2015).
- Tulloch, Phillips et al. (2012).
- Leslie (2014) Unpublished – Presented at the Australian DMA Clinical Pilates Summit, September 2014.
- Turner (2014) Unpublished – Presented at the Australian DMA Clinical Pilates Summit, September 2014.
- Rybak (2006).
- Calancie B, Needham-Shropshire B, Jacobs P, Willer K, Zych G, Green BA (1994). Involuntary stepping after chronic spinal cord injury. Evidence for a central rhythm generator for locomotion in man. Brain 117(Pt 5):1143–1159.
- Leslie (2015).
- Brown et al. (2017).
- Raysmith and Drew (2016).
- Drew, Raysmith, and Charlton (2016).

{kind=link}