How to Assess an Athlete’s Direction Bias and Use It to Improve Performance


Summary
Knowing your athlete’s direction bias can help improve motor control, direction of force application, and proprioception all through a few exercises you can incorporate into a warm up. Gym programming design can then use direction bias to help make an athlete more robust across all planes of movement while avoiding aggravating positions.
Knowing your athlete’s direction bias (DB) can help improve motor control, the direction of force application, and proprioception all through a few exercises you can incorporate into a warm up. Gym programming design can then incorporate DB to make an athlete more robust across all planes of movement while keeping them away from aggravating positions. If we look at movement quality as a central nervous system (CNS) instruction that avoids aggravating a sub-threshold pathology, then DB gives us our answer.
I previously wrote the article, “Direction Bias Gym Programming and Athletic Performance” outlining preliminary research and theories behind its use in the sports performance domain. This led to great interest in a common question: “How do I determine an athlete’s direction bias?” Apparently, I put the cart before the horse. This article provides a step by step approach on how to perform a basic DB assessment.
What is an Athlete’s Direction Bias and Why Do We Need to Know It?
First, let’s summarize what DB is, so we understand the implications of working it into an athlete’s programming.
- The body has a preferred way of moving that it finds most efficient, which results in improved quality of movement and power development called direction bias (or direction preference).
- DB is brought about by either:
- an underlying pathology (symptomatic or asymptomatic); or
- developmental reasons, which can be assessed quite easily with repeated movement testing in a DB assessment.
- If the athlete works either in a position or movement direction against their bias, they will inevitably:
- lose form
- find the exercise harder than it should be
- develop symptoms
All in all, these effects will yield a less than satisfactory training effect.
We determine DB by observing a person’s movement quality in three standardized dynamic stability tests before and after the same “repeated movement in one direction.” DB assessment is highly reliable and allows for assessing an asymptomatic individual as well as an athletic population. The hypothetical mechanism of action that improves function is based on Mackay-Lyon’s review.1 It’s believed to address the afferent input of pathology that affects locomotion’s regulating central pattern generator output.1,2Through direction-specific movement, therefore, the motor deficits induced by the pathology can improve.3
How to Perform a Direction Bias Assessment
This is what separates a therapy from an exercise: the ability to assess for change before and immediately after the intervention. DB assessment allows the therapist or coach to confidently prescribe an exercise as a therapy due to its validated, predictable response.
Direction bias assessment lets us confidently prescribe an exercise as a therapy. Share on XWe base DB assessment on the visual assessment of an athlete’s movement quality in:
- 5 single leg heel raises (5HR) on each leg
- 5 single leg squats (5SLS) on each leg
- 5 single leg hops (5SLH) on each leg
Give instructions as follows:
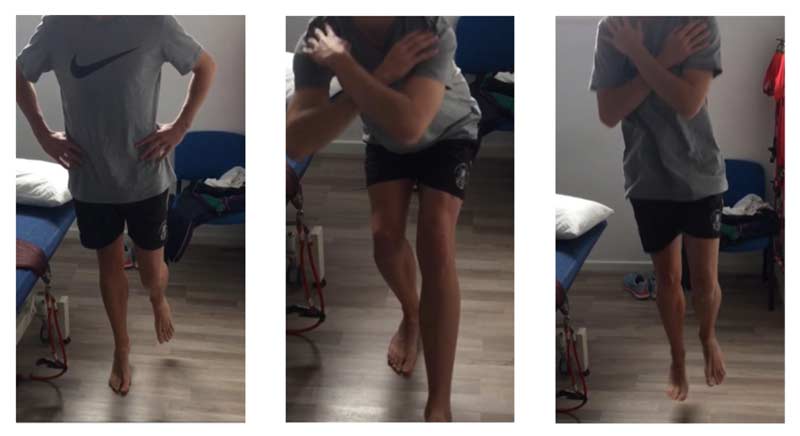
- 5HR—Fold arms across chest. Raise up and down on toes smoothly without stopping at top or bottom. Try to keep balanced on the one leg.
- 5SLS—Fold arms across chest. Bend the knee and lower slowly to a point as low as you feel comfortable, then raise back to upright without stopping at the top or bottom. Try to keep balanced on the one leg.
- 5SLH—Fold arms across chest. Hop five times in a row. Imagine you’re hopping on hot coals. Try to hop as high as possible but contact the ground for the shortest time possible for each hop. Try to keep balanced.
Ask the athlete to rate their baseline performance out of 5 on a 10-point scale for each test.
| Pre-Intervention | ||
| Left | Right | |
| Single leg heel raise | 3.5/5 | 2.5/5 |
| Single leg squat | 4/5 | 2/5 |
| Single leg hop | 3.5/5 | 2/5 |
| Total | 11/15 (73.3%) | 6.5/15 (43.3%) |
Frontal Plane
In our case example, the frontal plane displays poorer movement on the right side, which classifies the athlete as having a right sagittal plane bias. Subjective questions about an athlete’s past injury history will often show that, while perhaps asymptomatic at the time of testing, they report a more predominant injury history on that side. The correlation between injury history and movement dysfunction makes DB testing an invaluable tool for exercise prescription and potentially injury prediction modeling.4
In this case example, the athlete demonstrates a 30% difference in the Asymmetry Index across these tests. In itself this is worthy of attention; studies demonstrate that an asymmetry of greater than 20% in kinetic impulse with jumping can indicate a high risk of injury.5This protocol is currently under validation against a gold standard in a clinical trial, but anecdotal data is extremely favorable. And the ease of measure for the coach and clinician make it useful as a clinical tool by itself.
Sagittal Plane
Whether to choose a repeated extension or a repeated flexion intervention is a clinical judgment. We can determine this by doing the following, in order of importance:
- Ask the athlete if any positions make them sore or stiff consistently. Excessive bending is a flexion movement at the pelvis and lumbar spine. If this were sore, such as following a block session from sprinters, it would be an aggravator. It would make sense to choose the opposite movement of extension to provide the athlete a therapeutic effect.
- Ask the athlete about the mechanism of how their most significant past injury occurred. If the athlete injured their hamstring as they lunged toward the finish line, this indicates that flexion was the mechanism of injury so you would choose an extension movement to try and provide a therapeutic effect.
- Ask the athlete if there are any positions they prefer to be in when sore? If sleeping on their stomach is comfortable, this indicates that extension is an “easing” position, so you would choose an extension movement to try and provide a therapeutic effect.
The experienced clinician can draw upon familial and genealogical history as well as training response to select movements and injury history. However, if you’re unable to make a clinical determination from these questions about which direction to do the repeated movement exercise, simply choose one and let your re-assessment findings guide your DB determination.
To correlate the DB assessment findings, we also tend to add a physiological test to the data sample such as lumbar flexion and extension or straight leg raise (SLR) testing. Note that physiological testing tends to indicate a negative response if the repeated exercise is against the athlete’s DB or is an aggravator. However, it does not necessarily indicate a positive correlation if the physiological test improves. The triage of movement quality tests I’ve described is more sensitive to these changes.
| SLR | Right 70 degrees, Left 90 degrees |
| Lumbar Extension | 5 degrees restricted by discomfort |
Subjectively, this athlete reported his “first most significant injury” as a right hamstring injury at take off in the long jump. It’s a rapid hip and back extension movement, so we chose a repeated flexion bias exercise as the one most likely to be therapeutic.
How Do I Select the Intervention Exercise?
The DMA Clinical Pilates course suggests that the best exercises for testing an athlete’s DB are the following:
For Flexion Bias

Image 2. Roll-ups. The athlete maintains their sagittal plane bias leg in 45 degrees hip flexion. They can use momentum to roll up into a traditional sit-up position keeping the other leg down and reaching forward as far as their trunk can flex. They then return to the lying position by tucking their chin in and posterior pelvic tilting to slowly roll down as they breathe out. They repeat this 2 x 10-15.
Image 3. Heel touch. The athlete starts on their back with both hips flexed to 45 degrees. Instruct them to lift their bias leg up to 80 degrees hip flexion with both the arms and head as they breathe in. Then lower arms and head to the bed as they breathe out. Repeat this 2 x 15.
For Extension Bias

Image 4. Single leg kick. The athlete lies prone and shifts legs toward the bias side. Instruct them to rapidly “bend the knee, lift the hip, straighten the knee, and lower it controlled.” They repeat this 2 x 10.
Image 5. Four-point extension. The athlete starts on their hands and knees with hands under shoulders and knees under hips. Instruct them to lift and straighten their bias side leg, trying to make it “as long as possible.” Encourage them to try to keep their pelvis level and not laterally shift as they extend their leg and return. They repeat this 2 x 10.
In our case example, our long jump athlete performed 2 x 15 roll-ups and 2 x 15 heel touches moving his right leg. We then retested his repeated movement tests.
| Post-Intervention | ||
| Left | Right | |
| Single leg heel raise | 4/5 | 4/5 |
| Single leg squat | 4/5 | 4/5 |
| Single leg hop | 4/5 | 3/5 |
| Total | 12/15 (80%) | 11/15 (73.3%) |
| SLR | Right 90 degrees, Left 95 degrees |
| Lumbar Extension | 30 degrees no discomfort |
In this case, the asymmetry reduced from 30% to 6.7% and visually, overall movement quality and functional tests improved. If we were to do a crossover study with this athlete, we would see a deterioration of performance if they were to perform repeated right extension bias exercises such as the single leg kick or four-point extension described above.
We use this frequently to “prove” that we chose the correct bias by showing deteriorating performance with the anti-bias and then improving it again with the correct bias type exercises. It creates buy-in by the athlete and coach and helps prove in your mind that you’ve selected the right exercise intervention.
How Important are Asymmetry Changes?
The arguments regarding how important it is to correct asymmetry are not within this article’s scope. However, it’s hard to argue against a desire to improve the direction of force application, as demonstrated in these tests by repeated hopping over a set position or joint proprioception. The degree of how much a therapist or coach chases this utopia is certainly more than a worthwhile discussion.
Should I Use Direction Bias Assessments with My Athletes?
I love the phrase “athlete specific before sports specific” because it encapsulates the reasoning behind the sometimes unusual exercise selections that make up the programming. If an athlete moves badly in an exercise, sometimes it’s too difficult or time-consuming to coach them out of it. This is likely due to a CNS “protection mode” or “alarm theory” that prevents one from moving into a position that could be potentially deleterious with a load. The statement “the body is only as strong as the brain feels safe” describes this perfectly.
Although there is a huge amount of research still to be done in this area, I encourage you to try and find your athlete’s DB and learn how to use the intervention exercises in warm-ups and exercise selection to improve movement quality and performance and reduce injury risk.
DB assessment is taught as part of the DMA Clinical Pilates Courses for health professionals in Australia, and I highly recommend anyone with the opportunity to attend one of these courses. For more information beyond the scope of this report, I recommend reading the 2012 article by Tulloch and Phillips as well as these DMA Clinical Pilates courses.
References
- Mackay-Lyons, M. (2002) Central pattern generation of locomotion: A review of the evidence. Physical Therapy, 82(1): 69-83.
- Phillips, C. (2015) Avoiding paralysis by analysis makes complex patients simple. Presented at 2015 Australian Physiotherapy Association Conference, Gold Coast. October 2015.
- Wajswelner, H., B. Metcalf, et al. (2012) Clinical Pilates versus general exercise for chronic low back pain: randomized trial. Medicine and Science in Sport and Exercise, 44(7): 1197-1205.
- Kiesel,K; Butler, R; Plisky, P (2014). Prediction of Injury by limited and asymmetrical fundamental movement patterns in American football players. Journal of SportRehabilitation,23(2): 88-94.
- Jordan MJ, Barnert J, Aagaard P, Herzog W. (July 13, 2015). The kinetic impulse asymmetry index in the vertical jump predicts lower bodyinjury in elite athletes. In: XXV Congress of the International Society of Biomechanics Abstract Book. Glasgow, United Kingdom. (pp. 664-665) (AS-0311).

{kind=link}