



Information about groin injuries is not as accessible as information about hamstring injuries and is likely more complicated. Unlike hamstrings, which are clearly defined, the groin is a messy area with a large array of muscle groups in the lower pelvic area.
And, while muscles are uniquely connected, soft tissue does not have origins and insertions, making matters more complicated. Fascia does have some connections to muscle chains, but, aside from electromyography (EMG) readings, science isn’t clear about what occurs with fascia.
Adding to the confusion is a major disconnect about groin injuries among coaches, manual therapists, surgeons, and even physical therapists in the sports medicine community.
The good news is that many great experts, including Kristian Thornborg, are helping to clarify how to battle groin injuries by providing specific information to empower coaches who are on the first line.
This article summarizes various presentations given at international conferences and workshops about athlete groin injuries. I will share common mistakes along with practical and effective alternatives.


Teams Continue to Use the General Groin Landmark
For simplicity, I’ll share the four regions that groin experts consider to be part of the anatomy family, and I’ll include patterns occurring in sport.
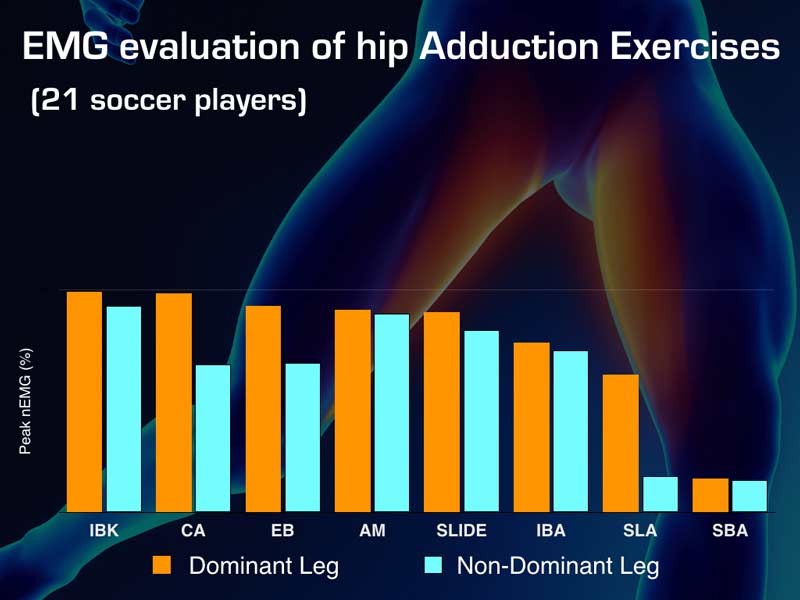
- Adductor. This muscle group is a common problem for hockey and soccer athletes, although any sport can have issues here. At medical symposiums, there’s a lot of interest in how to treat this area.
- Abdominal. The abdominal region is a nebulous area, and the terminology used for describing associated problems are changing. Anytime name changes occur, we can interpret this to mean “we don’t know what is going on” and brace ourselves for frustrating times ahead.
- Hip Flexor. Muscle groups, including the psoas major (sometimes minor), that drive femoral flexion of the hip are considered hip flexors. With some athletes, locomotion with EMG shows that muscles in addition to the psoas major are used during the recovery phase.
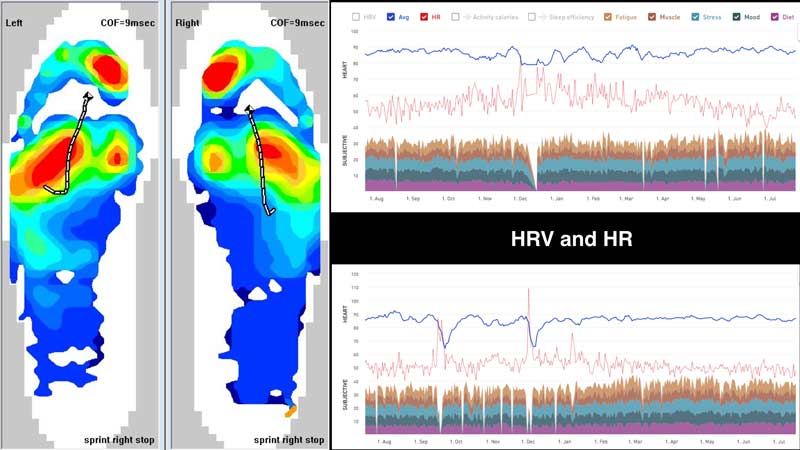
- Hip Joint. Labrums are all the rage now. When an athlete complains of deep pain in the pelvis, they feel pressured to seek treatment. I have one athlete with systemic inflammation who felt pain during heavy academic periods, usually in late season of his sport. Our first fear was hip problems. I used blood analysis and Heart Rate Variability (HRV) monitoring and clearly saw his sleep and study balance was disrupted. He needed more rest.
I follow the parameters given by medical professionals and have room to experiment and train. I don’t like working with someone without a very precise diagnosis. By this, I mean specific location and etiology.

And this is the solution. We must obtain a complete and confident assessment of the injury location and etiology. Simply labeling anything above the knee and below the navel as the groin is not useful.
I’m amazed how much “groin” tagging occurs with medical athlete monitoring system (AMS) data. And I’ve found it frightening when injury models from software vendors don’t use classic protocols that have passed the test of time. Willem van Mechelen provided great concepts that are useful now and were ahead of their time when he developed them. He used terminology that was very contemporary and appropriate.

Teams Don’t Plan Practices to Avoid Soft Tissue Injuries
David Tenney, director of performance and sports science with the Seattle Sounders, has shared his experience using simple player tracking data to visualize issues with deceleration (adductor and possible joint) and high-speed metrics that can show why athletes pull hamstrings.
While this system is binary and not very sophisticated, it’s a great place to start for teams when beginning to design their practices. I’ve seen a pattern develop from my team visits. Coaches struggle to meet the demands of tactical strategies while trying to harmonize practice with the physiological and musculoskeletal demands on their athletes.


The high-performance experts of the NFL and NCAA football are experimenting with ramping up practices to potentiate for game day. I don’t believe the hype. Teams amp up for competition regardless of whether they snatched light during the 24-48 hours before a game. The art is coming into a game fresh (rested), and fit (conditioning maintained). Not flat (not sharp).
Here are four basics of practice design. At first glance, they look remedial. But many programs chase the small sexy details and fail to address the key components.
- Volume. Occasionally too much is too much. No matter how you cut it up, it’s still too much to swallow. My favorite line of one NFL strength coach talks not about metrics but the need to get off the field. If athletes are breaking down, we need to stop using recovery methods to mask problems and just take them off the practice field.
- Distribution. Derek Hansen has talked about the dead zone; the comfortable, moderate intensity area of training that doesn’t provide much stimulation and doesn’t produce fatigue but also doesn’t help athletes progress. Polarized training is hard to incorporate for team sports where high-speed plays are rehearsed. Some days are best for recovery work and aerobic activities. For example, practices following games and during off days. Clear messages to the body are instrumental in keeping fit and nurturing improvement.
- Allocation. Most strength coaches are stuck with little time and athletes who are spent of energy to perform lifting. After every practice, athletes must walk off the field with two units of gas in the tank. Team coaches must save one unit for lifting and other off-field work and one unit to reduce the risk of residual fatigue from the practice week.
- Sequence. Creating an order to training sessions to cover both the X’s and O’s of strategy and human skill is a difficult art. Working backward, I believe, is the smartest option. Tweaking speeds and volumes of work to keep athletes stay sharp and without fatigue is a fine narrow line.
More specific options exist, of course, that are beyond this article’s scope. The main takeaway is to start with priorities and then move to details that, by themselves won’t move the needle, but collectively will create progress.

Teams Don’t Embrace MyoAnalytics and Don’t Track Muscle Recruitment
When dealing with muscle injuries, skip the middleman and test the muscles. Avoid using proxy metrics. Injuries often slip past these screens because they’re used for convenience instead of more direct but cumbersome methods. Rather than only doing Rate of Perceived Exertion (RPE) and subjective questionnaires, it’s better to outsource expertise and receive inconvenient data. Or make it easier to obtain valuable data.

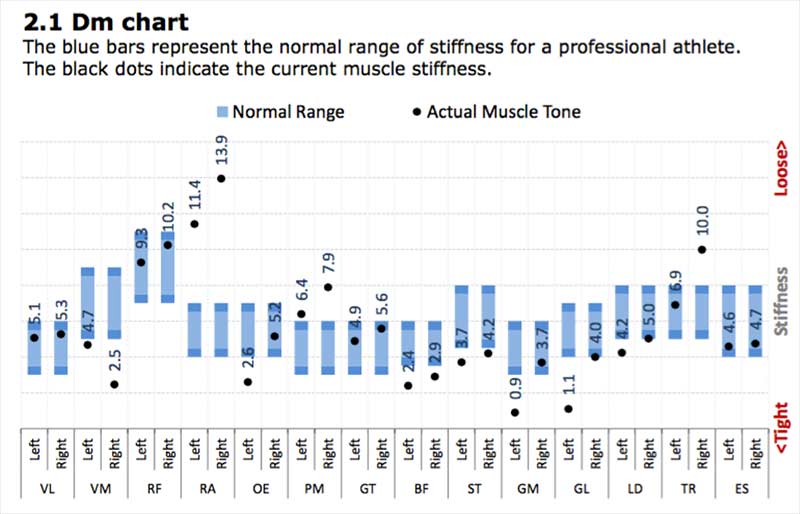
EMG, MyoAnalytics, and electronic muscle stimulation (EMS) create the Trinity of muscle tracking. EMG looks at recruitment, MyoAnalytics shows changes caused by fatigue, and EMS can help keep athletes, who are limited in training, get more from their less frequent workouts. For pro teams, I suggest EMS.
Finally, unless teams suffer no injuries, murder their competition, and play undefeated for years, don’t compare more successful teams to less successful teams as evidence of results. One year is not an example of a sustainable system, just a possible outlier of young healthy talent or trading away “injury prone” athletes.

Teams Train Their Athletes Like Senior Citizens or Use Spanish Inquisition Torture
Although middle ground for conditioning is not good, staying in the middle ground for therapy and training moderation is great medicine. I’ve seen abusive manual therapy where tendons are traumatized because some therapists believe it’s the “poor man’s PRP (post platelet-rich plasma).”
Bruising and other manual therapy effects are common, and the therapy has no scientific support. Addressing tone is real, but elbows digging into areas and creating hematomas is excessive. On the other hand, we have some teams treating athletes like delicate china, and this needs to stop also.
I am active but don’t train. When I see guys watching a video of a basketball athlete doing trap bar deadlifts with 315 pounds like it’s magic, I’ll walk over and use old man strength to humble the achievement.
Having our elite athletes perform high-volume TRX lunges and push-ups on their knees is a joke. As a coach, I’m not looking for world-class powerlifting or weightlifting numbers. I’m looking for exercises that improve performance backed by science.
The kBox offers a great solution for coaches wanting to develop eccentric abilities that matter rather than squeezing Nerf balls. A rigorous blend of lateral and split squats are valuable ways to help stabilize the pelvis and move forces through the center of mass more efficiently.
On Twitter, I followed a link: eccentric strength linked to a reduction in groin injuries. I found many shares by therapists with exercises that would rot an athlete’s strength by babysitting them with bodyweight and elderly man training.
Progressive overload is not dated, it’s essential. If we ignore it, we’ll just be stuck in the mud. Here are three basic checklist items we must ask every year when working with the same, or similar, athletes.
- Do I provide the same amount of training time in the weight room as previous years?
- Are my athletes coming in as strong and fast as the beginning of last season?
- Does the decay of power decrease from baseline each year or does it accelerate?
I know this is simplified. Unfortunately, many coaches skirt around the issues that drive change.
The first question addresses the tough reality of having access to improving or, at least, maintaining strength. The second question emphasizes the off-season as the time when champions are made. If management knows athletes are coming in less prepared, someone other than the fitness or strength coach needs accountability.

Many teams breakdown and wear out from too much competition and too little preparation. We all know this. The keys to each competition rest on which team is less skilled or decays the least from fatigue and loss of power.
We can win by focusing on beating the opponent and not following utopian models found in old Olympic literature from Eastern bloc countries. Remember the story about the two campers getting ready for bed. One decides to put on sneakers to get ready for the grizzly bear. The other camper explains, “You can’t outrun bears that move at 30 miles per hour.” The sneaker-clad camper answers, “I only have to outrun you!” The moral of the story is the same with strength in team sports. All we can try to do is beat the competition by doing what we can, not by chasing perfection.

Teams Don’t Use Sports Podiatry Correctly, If at All
Sports podiatry gets a bad rap because most coaches think only about orthotics or surgery. With pressure mapping and EMG, I’ve seen how sport adaptations and an athlete’s anatomy can increase recruitment of secondary muscles not designed for locomotion.
When athletes run fast, they need silence periods, times when muscles turn off. Otherwise, injuries can cause either constant firing for protection (guarding) or altered ground reaction forces through the foot and ankle complex.
With highly sophisticated software modeling and novel data collection, we’re seeing a silent epidemic. Many combinations of foot structure, foot function, and fatigue are increasing muscle and joint injuries.

All of the variables make it nearly impossible for us coaches to decipher. For years I’ve been using experts who cover these variables, and they’ve solved complex “injury prone” athletes like a Sherlock Holmes murder mystery.
Here are a few ideas teams should implement with their teams to reduce injuries. Athletes must be treated like Formula 1 racecars. Many involved in elite sport love this analogy for PowerPoint presentations. But I don’t see the “tire data.”
I spoke at the 2015 FLIR InfraMation Conference where the Red Bull racing director explained the value of tire technology and thermography. I believe sports that involve running must treat their athletes’ feet like motorsport tire technology.
Sports that involve running must treat their athletes’ feet like Formula 1 tire technology. Click To TweetHere is what we can do better with Sports Podiatry:
- Anatomy. New modeling and imaging can create 3D renderings of the feet. Foot anatomy is very complicated, and it’s very difficult to manage and calculate force transfer. Classic techniques paired with modern technology can do a great job here.
- Function. Clinical evaluation tests the foot’s function, focusing on joint range and mobility.
- Pressure Profile. The actual center of pressure and force-time curves can tease out slight patterns that can create changes in muscle recruitment. This alone will not provide a definitive compass for injury, but it is a factor that helps.
- Shoe Design. Each cleat or sneaker must be scored as to how it interacts with the forces of locomotion and different foot forces. Most teams, except some high-level football clubs and rugby teams, do a poor job with shoe design evaluation for their players.
Obviously, the above suggestions are not comprehensive. Simply addressing them, however, helps reduce the likelihood of injury-causing alterations with muscle recruitment. Following any of these suggestions will be a great start.
Build Your Own Checklist
The goal is to create a checklist that identifies factors and addresses areas of increased risk. If teams continue to use AMS software and effective measurement tools to obtain the appropriate data, more data mining will reveal the small factors that add up to injury patterns.
Each checklist includes sub-checklists that create a perfect infrastructure roadmap to reduce injuries. Hopefully, this skeleton outline will then be fleshed out by specialists so groin injuries can be reduced.
Since you’re here…
…we have a small favor to ask. More people are reading SimpliFaster than ever, and each week we bring you compelling content from coaches, sport scientists, and physiotherapists who are devoted to building better athletes. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — SF
Suggested Reading
- Van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med 1992; 14:82-99.
- Hölmich P, Thorborg K, Nyvold P, Klit J, Nielsen MB, Troelsen A. Does bony hip morphology a ect the outcome of treatment for patients with adductor- related groin pain? Outcome 10 years after baseline assessment. Br J Sports Med. 2014;48:1240-1244.
- Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. Am J Sports Med 2010;38:2051–7.
- Thorborg K, Serner A, Petersen J, et al. Hip adduction and abduction strength profiles in elite soccer players: implications for clinical evaluation of hip adductor muscle recovery after injury. Am J Sports Med 2011;39:121–6.

Another mistake is not to use simple groin injury prevention programs that have been proven effective
http://bjsm.bmj.com/content/early/2018/06/08/bjsports-2017-098937